
Acute Pancreatitis
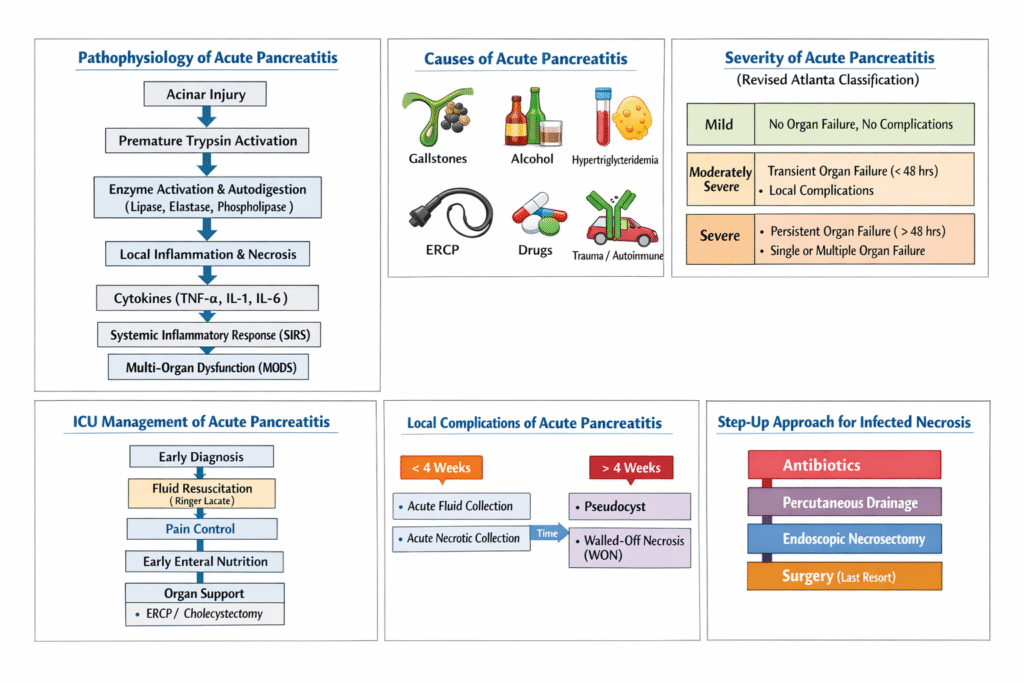
Acute Pancreatitis is an acute inflammatory process of the pancreas caused by premature activation of pancreatic digestive enzymes leading to autodigestion, inflammation, edema, necrosis, and systemic inflammatory response.
It ranges from:
- Mild self-limiting interstitial edema
to - Severe necrotizing pancreatitis with multiorgan failure.
Diagnostic Criteria (Revised Atlanta Classification)
Diagnosis requires 2 of 3 criteria:
Criteria | Details |
1. Typical abdominal pain | Acute severe epigastric pain radiating to back |
2. Elevated pancreatic enzymes | Lipase or amylase >3× upper limit |
3. Imaging findings | CT/MRI/USG compatible with pancreatitis |
Differential Diagnosis
Condition | Key Difference |
Perforated ulcer | Free air |
Acute cholecystitis | RUQ dominant |
Mesenteric ischemia | Severe pain/lactate |
MI | ECG/troponin |
Aortic dissection | Tearing pain |
Etiology
Remember:“I GET SMASHED”
Most common causes:
- Gallstones
- Alcohol
Cause | Examples |
I | Idiopathic |
G | Gallstones |
E | Ethanol |
T | Trauma |
S | Steroids |
M | Mumps/malignancy |
A | Autoimmune |
S | Scorpion sting |
H | Hypertriglyceridemia/hypercalcemia |
E | ERCP |
D | Drugs |
Common Causes
1. Gallstone Pancreatitis
Most common overall cause.
Mechanism:
- Transient obstruction of ampulla
- Bile reflux
- Pancreatic duct obstruction
Suggestive features:
- Female
- Obesity
- RUQ pain
- Elevated ALT (>150 IU/L strongly suggests biliary cause)
2. Alcoholic Pancreatitis
Mechanisms:
- Direct acinar toxicity
- Protein plug formation
- Oxidative stress
Typically occurs after years of drinking.
3. Hypertriglyceridemia
Usually TG >500 mg/dL
High risk >1000 mg/dL
Mechanism:Toxic free fatty acid release
Clues:
- Lactescent serum
- Diabetes
- Obesity
4. Drug-Induced Pancreatitis
- Azathioprine
- Valproate
- Didanosine
- Thiazides
- Furosemide
- GLP-1 agonists
- DPP4 inhibitors
- Estrogens
5. Post-ERCP Pancreatitis
Risk factors:
- Difficult cannulation
- Sphincterotomy
- Female sex
- Sphincter of Oddi dysfunction
Prevention:
- Rectal NSAIDs
- Pancreatic duct stent
6. Hypercalcemia
Causes:Hyperparathyroidism,Malignancy
Mechanism:Intrapancreatic trypsin activation
7. Autoimmune Pancreatitis
Associated with:IgG4 disease
Features:
- Painless jaundice
- Diffuse enlargement
- Steroid responsive
Pathophysiology
Central Event:
Premature activation of trypsinogen → trypsin inside pancreas.
Trypsin activates:Elastase/Phospholipase/Lipase
Result:Fat necrosis/Vascular injury/Hemorrhage/Cytokine storm
Systemic Pathophysiology
Massive cytokine release:TNF-α/IL-1/IL-6
Leads to:SIRS/Capillary leakARDS/ShockAKI/MODS
TYPES
1. Interstitial Edematous Pancreatitis
- Most common
- Mild inflammation
- Good prognosis
2. Necrotizing Pancreatitis
- Pancreatic necrosis
- Peripancreatic necrosis
- Infected necrosis possible
Clinical Features
Pain
Classic:
- Sudden severe epigastric pain
- Radiates to back
- Worse supine
- Better leaning forward
Associated Symptoms
- Nausea
- Vomiting
- Fever
- Abdominal distension
- Ileus
Examination Findings
Finding | Significance |
Tachycardia | Hypovolemia/SIRS |
Fever | Inflammation/infection |
Hypotension | Severe disease |
Epigastric tenderness | Common |
Guarding | Severe inflammation |
Jaundice | Gallstones |
Reduced bowel sounds | Ileus |
Hemorrhagic Signs
Rare but severe.
Sign | Description |
Cullen sign | Periumbilical ecchymosis |
Grey-Turner sign | Flank ecchymosis |
Fox sign | Groin ecchymosis |
Suggest hemorrhagic pancreatitis.
Laboratory Diagnosis
Serum Amylase | Serum Lipase |
Less specific for pancreatitis | More specific for pancreatitis |
Rises within 6–12 hours | Rises within 4–8 hours |
Peaks at 24–30 hours | Peaks at about 24 hours |
Returns to normal in 3–5 days | Remains elevated for 8–14 days |
Can be normal in hypertriglyceridemia-induced pancreatitis | More reliable in hypertriglyceridemia |
May rise in intestinal ischemia, perforation, ectopic pregnancy, renal failure | May rise in renal failure, bowel ischemia, cholecystitis |
Macroamylasemia can falsely elevate level | No macro-lipasemia equivalent commonly significant |
Macroamylasemia and Macrolipasemia
These are benign biochemical conditions in which pancreatic enzymes bind to large molecules (usually immunoglobulins), forming high-molecular-weight complexes that cannot be easily filtered by the kidneys.
This leads to:
- Persistently elevated serum enzyme levels
- Reduced urinary excretion
- No true pancreatic injury
Other Labs
Test | Importance |
CBC | Hemoconcentration/leukocytosis |
LFTs | Gallstone cause |
ALT >150 | Strong biliary predictor |
Calcium | Hypocalcemia severity |
Triglycerides | HyperTG pancreatitis |
CRP | Severity marker |
ABG | Hypoxemia/metabolic acidosis |
Lactate | Shock severity |
Imaging
1. Ultrasound
First imaging in all patients.
Purpose:Detect gallstones/CBD dilation
Limitation:Pancreas poorly visualized due to gas
2. Contrast CT Abdomen
Best for:Necrosis/Complications/Severity assessment
Not needed routinely at admission.
Ideal timing:After 72 hours if severe/not improving.
CT-Based Severity Assessment in Acute Pancreatitis
Feature | Balthazar Grading | CT Severity Index (CTSI) | Modified CT Severity Index (MCTSI) |
Purpose | Describes morphologic severity on CT | Combines Balthazar grade + necrosis | Simplified and clinically superior modification |
Main Components | Pancreatic inflammation and collections | Inflammation + necrosis | Inflammation + necrosis + extrapancreatic complications |
Necrosis Included? | No | Yes | Yes |
Extrapancreatic Complications Included? | No | No | Yes |
Maximum Score | Grade A–E | 10 points | 10 points |
Best Use | Morphologic description | Severity prediction | Modern preferred CT severity scoring |
Balthazar Grading
Grade | CT Findings | Points in CTSI |
A | Normal pancreas | 0 |
B | Focal/diffuse enlargement | 1 |
C | Peripancreatic inflammation | 2 |
D | Single peripancreatic fluid collection | 3 |
E | ≥2 fluid collections OR gas in pancreas/retroperitoneum | 4 |
Pancreatic Necrosis Scoring (Used in CTSI)
Extent of Necrosis | CTSI Points |
None | 0 |
<30% | 2 |
30–50% | 4 |
>50% | 6 |
CT Severity Index (CTSI) Formula=Balthazar Score+Necrosis Score
CTSI Score | Severity | Mortality/Complications |
0–3 | Mild | Low |
4–6 | Moderate | Intermediate |
7–10 | Severe | High |
Modified CT Severity Index (MCTSI)
Components
Parameter | Score |
Pancreatic inflammation | 0–4 |
Pancreatic necrosis | 0–4 |
Extrapancreatic complications | 2 |
MCTSI Detailed Scoring
Finding | Score |
Normal pancreas | 0 |
Intrinsic pancreatic abnormalities with/without inflammatory fat changes | 2 |
Pancreatic/peripancreatic fluid collection OR fat necrosis | 4 |
No necrosis | 0 |
≤30% necrosis | 2 |
>30% necrosis | 4 |
Any extrapancreatic complication | 2 |
Extrapancreatic Complications in MCTSI
Include:
- Pleural effusion
- Ascites
- Vascular complications
- GI involvement
- Parenchymal complications
MCTSI Interpretation
MCTSI Score | Severity |
0–2 | Mild |
4–6 | Moderate |
8–10 | Severe |
3. MRI/MRCP
Useful for:
- Biliary obstruction
- Duct evaluation
- Necrosis characterization
Revised Atlanta Classification
Severity Category | Definition / Features |
Mild Acute Pancreatitis | • No organ failure • No local complications • No systemic complications • Usually self-limiting with excellent prognosis |
Moderately Severe Acute Pancreatitis | • Transient organ failure (<48 hours) OR • Local complications (e.g., fluid collection, necrosis, pseudocyst) OR • Exacerbation of comorbid disease |
Severe Acute Pancreatitis | • Persistent organ failure >48 hours • May involve one or multiple organs • Respiratory failure • Renal failure • Shock/cardiovascular failure • Associated with high mortality risk |
Modified Marshall Scoring System in Acute Pancreatitis
Used in the Revised Atlanta Classification to define organ failure.
- Score ≥2 in any organ system = organ failure
- Persistent organ failure (>48 h) defines severe acute pancreatitis
Organ System | 0 | 1 | 2 | 3 | 4 |
Respiratory (PaO₂/FiO₂) | >400 | 301–400 | 201–300 | 101–200 | ≤100 |
Renal (Serum Creatinine mg/dL) | <1.4 | 1.4–1.8 | 1.9–3.6 | 3.6–4.9 | >4.9 |
Cardiovascular (Systolic BP mmHg) | >90 | <90, fluid responsive | <90, not fluid responsive | <90, pH <7.3 | <90, pH <7.2 |
Severity Scores
Score | Main Strength | Limitations | Current Role |
APACHE II | Most validated ICU severity score; dynamic and repeatable | Complex; many variables | Most accurate overall for predicting severe disease and mortality |
BISAP | Simple bedside early score | Slightly less accurate than APACHE II | Most practical early bedside score |
Ranson Score | Historically classic | Delayed (48 h), outdated | Mostly exam importance |
BISAP Score
Variable |
BUN >25 |
Impaired mental status |
SIRS |
Age >60 |
Pleural effusion |
Score ≥3:High mortality risk.
Initial Management
1.Fluid Resuscitation
Controlled Goal-Directed Fluid Therapy(WATERFALL Trial) – hydration in first 24 hrs
Preferred Fluid: Lactated Ringer’s (LR)
Advantages over normal saline:
- Less hyperchloremic acidosis
- Reduced inflammation
- Better pH balance
- Lower SIRS rates
Typical Regimen
- 5–10 mL/kg/hour OR Initial bolus:10–20 mL/kg if hypovolemic
- Maintenance:1.5–3 mL/kg/hr
Assessing Fluid Responsiveness
Clinical Parameters
- HR<120 ,BP≥65 mmHg
- Capillary refill <3
- Urine output >0.5ml/kg/hr
Parameter | Goal |
MAP | ≥65 mmHg |
Urine output | >0.5 mL/kg/h |
Hematocrit | Avoid rising |
BUN | Falling trend |
Why Avoid Excessive Fluids? Over-resuscitation causes:
- Abdominal compartment syndrome
- Pulmonary edema
- ARDS
- Increased mortality
2.Pain Management
Opioids
Commonly used:Fentanyl/Hydromorphone/Morphine
Old concern:“Morphine causes sphincter of Oddi spasm”
Current evidence:Clinically insignificant-Morphine acceptable
Multimodal Analgesia
May include:
- Paracetamol/Ketamine infusion
- Epidural analgesia (selected ICU patients)
3.Nutrition
Early Enteral Feeding(Within 24–48 hours if possible.)
Benefits:
- Preserves gut barrier
- Reduces infection
- Reduces bacterial translocation
–Diet-Low-fat solid diet(Fat thought to stimulate pancreas excessively.)
Route | Notes |
Oral | If mild and tolerated |
NG feeding | Usually adequate(NG feeding generally as effective as NJ feeding) |
NJ feeding | If gastric intolerance |
TPN only if enteral impossible.
4.Antibiotics
NOT routinely indicated
Do NOT give prophylactic antibiotics for sterile necrosis.
Indications
Only if:
- Infected necrosis
- Cholangitis
- Extrapancreatic infection(Pneumonia/UTI/CLABSI)
Signs of Infected Necrosis
- Fever
- Persistent sepsis
- Gas in necrosis on CT
- Positive culture
Antibiotics That Penetrate Pancreas
- Carbapenems
- Piperacillin-tazobactam
- Quinolones
- Metronidazole
Gallstone Pancreatitis Management
Urgent ERCP if:Cholangitis
OR Persistent biliary obstruction
Not needed routinely in all gallstone pancreatitis.
Hypertriglyceridemia Pancreatitis Treatment
- Insulin infusion
- Treat DKA if present
- Fibrates later
- Plasmapheresis in selected severe cases
Complications
Collection | Timing | Contents |
Acute peripancreatic fluid collection | <4 weeks | Fluid only |
Pancreatic pseudocyst | >4 weeks | Fluid only |
Acute necrotic collection | <4 weeks | Fluid + necrosis |
Walled-off necrosis | >4 weeks | Necrosis |
Management of Collections
Observation
Most asymptomatic collections require no treatment.
Drainage Indications
- Infection
- Gastric outlet obstruction
- Biliary obstruction
- Persistent pain
- Failure to thrive
Infected Pancreatic Necrosis
Major cause of late mortality.
Diagnosis
- Gas in collection on CT
- Clinical sepsis
- FNA rarely needed now
Management: Step-Up Approach
- Antibiotics
- Percutaneous/endoscopic drainage
- Minimally invasive necrosectomy if needed
Timing of Intervention
- Delay intervention whenever possible
- Ideally:≥4 weeks after onset
- Reason:Allows walling-off of necrosis.
Vascular Complications
Complication | Features |
Splenic vein thrombosis | Gastric varices |
Pseudoaneurysm | Massive bleeding |
Hemorrhage | Shock |
Pseudoaneurysm often:
- Splenic artery
- Gastroduodenal artery
Systemic Complications
System | Complication |
Respiratory | ARDS, pleural effusion(left>>right) |
Renal | AKI |
CV | Shock |
Hematologic | DIC |
Metabolic | Hypocalcemia |
GI | Ileus |
ARDS in Pancreatitis
Due to:Cytokine-mediated lung injury/Capillary leak
Major mortality contributor.
Abdominal Compartment Syndrome
Causes:Massive fluids/Ileus/Edema
Suspect if:
- Rising airway pressures
- Oliguria
- Tense abdomen
Measure bladder pressure.
AKI in Pancreatitis
AKI in pancreatitis is usually multifactorial.
Major Mechanisms
1. Hypovolemia (Most Important Early Cause)
Acute pancreatitis causes:
- Massive third spacing
- Vomiting
- Reduced oral intake
- Capillary leak
- Sweating/tachypnea
This leads to:
- Reduced renal perfusion
- Prerenal AKI
2. Systemic Inflammatory Response Syndrome (SIRS)
Result:
- Renal ischemia
- Acute tubular injury
3. Persistent Hypotension/Shock
Shock causes:
- Renal hypoperfusion
- Ischemic ATN
Septic shock may occur later due to:
- Infected necrosis
- Secondary infections
4. Intra-Abdominal Hypertension (IAH)