🔷 HEPATOPULMONARY SYNDROME (HPS)
📌 Definition (AASLD Criteria)
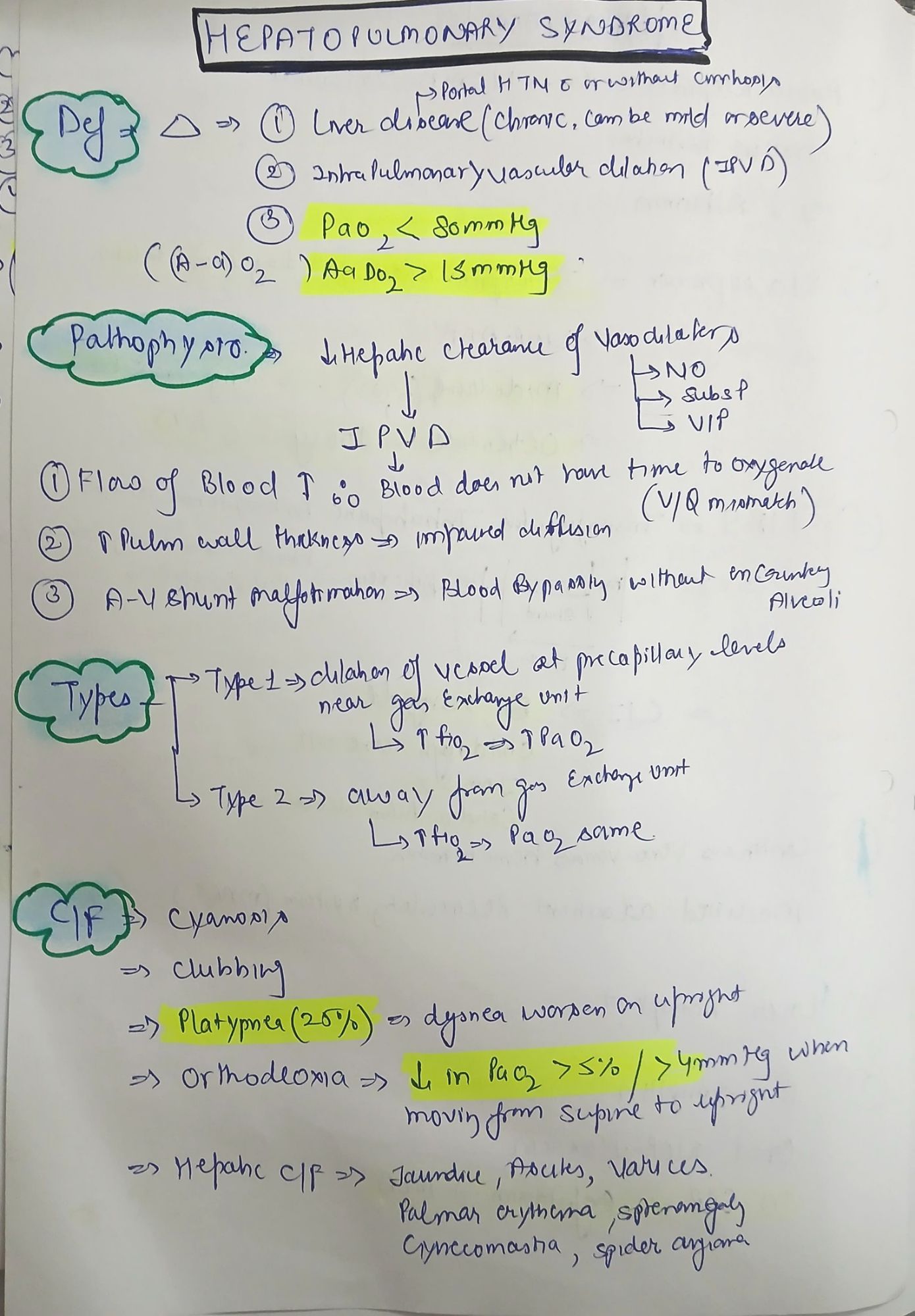
HPS is a triad of:
- Chronic liver disease and/or portal hypertension
- Arterial hypoxemia (PaO₂ <80 mmHg or A–a gradient >15 mmHg)
- Intrapulmonary vascular dilatations (IPVDs)
🔬 Pathophysiology
|
Mechanism |
Effect |
|
Portal hypertension → NO overproduction |
Systemic and pulmonary vasodilation |
|
Pulmonary capillary dilation |
↑ Capillary diameter → ↓ oxygen diffusion |
|
Right-to-left intrapulmonary shunt |
Bypasses alveolar oxygenation |
|
Ventilation-Perfusion (V/Q) mismatch |
Leads to hypoxemia |
|
↓ Hypoxic pulmonary vasoconstriction |
Contributes to shunt physiology |
🔑 Key mediators: Nitric oxide, endothelin-1, carbon monoxide, angiogenesis (VEGF)
🔬 Histopathology
- Dilated pulmonary capillaries (20–500 µm)
- Normal alveolar architecture
- Capillary remodeling without inflammation
🔍 Clinical Features
|
Feature |
Notes |
|
Platypnea |
Dyspnea worsens in upright position |
|
Orthodeoxia |
↓ PaO₂ ≥5% or ≥4 mmHg on standing |
|
Dyspnea, fatigue |
Progressive |
|
Clubbing, cyanosis |
In advanced stages |
|
Spider nevi |
Indicator of hyperdynamic circulation |
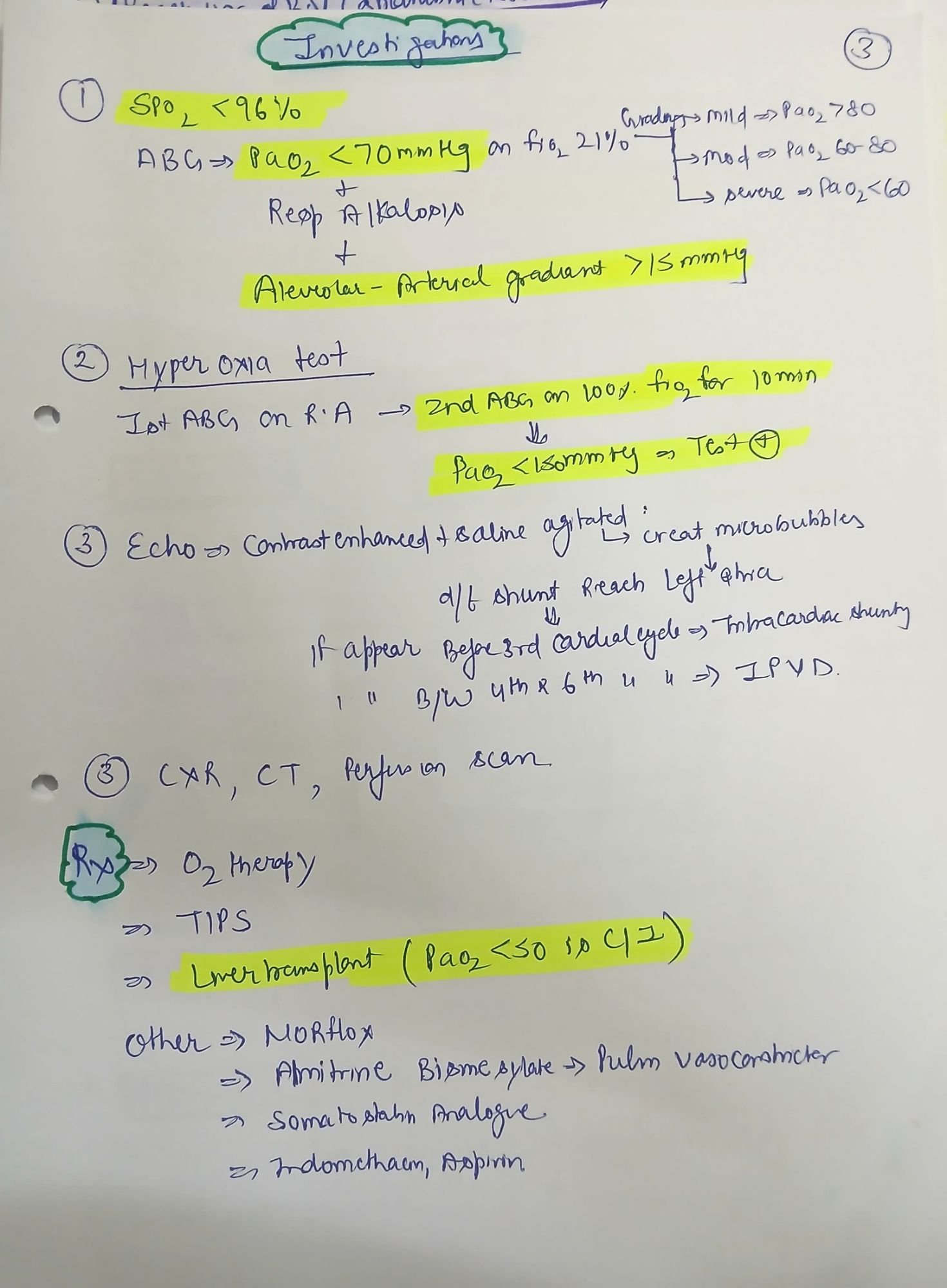
🧪 Diagnostic Work-up
|
Test |
Findings |
|
ABG |
↓ PaO₂, ↑ A–a gradient |
|
Pulse oximetry |
↓ SpO₂ on standing |
|
Contrast-enhanced TTE |
Bubbles appear in left atrium after 3–6 beats (vs. <3 beats in PFO) |
|
99mTc-MAA scan |
Uptake in brain/kidneys → intrapulmonary shunt |
|
CT Chest |
Shows diffuse vascular dilations |
|
Liver function tests |
Often deranged |
🔎 Severity Classification (by PaO₂)
|
Severity |
PaO₂ (mmHg) |
|
Mild |
≥80 |
|
Moderate |
60–79 |
|
Severe |
50–59 |
|
Very severe |
<50 |
💉 Management
🧬 Medical
|
Option |
Remarks |
|
Oxygen therapy |
Mainstay for symptom relief |
|
NO inhibitors (methylene blue) |
Temporary benefit |
|
Pentoxifylline |
TNF-α blocker |
|
Garlic extract |
Vasomodulator |
|
Somatostatin analogs |
In trials |
📌 No medical therapy reverses disease long-term.
🩺 Liver Transplantation
- Only definitive therapy
- ~85% resolution post-transplant (within 6–12 months)
- High MELD exception score allowed for HPS
🛑 Contraindications
- PaO₂ <50 mmHg may be a relative contraindication to transplantation due to increased perioperative mortality.
📚 Key Points for Exams
- Triad: Liver disease + IPVD + hypoxemia
- Diagnostic test of choice: Contrast-enhanced transthoracic echo (bubble study)
- Definitive treatment: Liver transplantation
- Differentiator from PoPH: HPS has low PVR, normal/low PAP
🔷 PORTOPULMONARY HYPERTENSION (PoPH)
📌 Definition (as per 6th WSPH)
PoPH = Pulmonary arterial hypertension (PAH) + portal hypertension, defined by:
|
Hemodynamic Parameter |
Threshold |
|
mPAP |
>20 mmHg |
|
PVR |
>2 Wood units |
|
PAWP |
≤15 mmHg |
|
Portal hypertension |
Clinically evident (with/without cirrhosis) |
🔬 Pathophysiology
|
Mechanism |
Role |
|
Shear stress from hyperdynamic circulation |
Endothelial injury |
|
Imbalance: ↑ vasoconstrictors (endothelin-1), ↓ vasodilators (NO) |
Vasoconstriction, remodeling |
|
Smooth muscle hypertrophy |
↑ PVR |
|
Intimal fibrosis |
Fixed PAH |
⚠️ Distinct from HPS, which is vasodilation dominant.
🔍 Clinical Features
|
Feature |
Notes |
|
Dyspnea |
On exertion, then at rest |
|
Fatigue |
Common early symptom |
|
Syncope |
Indicates severe disease |
|
Signs of RV failure |
JVP, ascites, edema |
|
Loud P2 |
Pulmonary hypertension sign |
🧪 Diagnosis
📉 Echocardiography
- RV hypertrophy/dilation
- Elevated RV systolic pressure
📏 Right Heart Catheterization (Definitive)
|
Parameter |
Threshold |
|
mPAP |
>20 mmHg |
|
PAWP |
≤15 mmHg |
|
PVR |
>2 WU |
📈 Additional Tests
- NT-proBNP: Elevated in RV strain
- LFTs: For MELD
- V/Q scan: Rule out CTEPH
- CXR: Enlarged PA, pruning
- CT: Enlarged main PA (>29 mm), RV enlargement
💊 Treatment
🚨 General
- Avoid volume overload
- Sodium restriction, diuretics
- O₂ for hypoxemia
- Avoid hepatotoxic or cardiodepressive drugs
💉 Specific PAH Therapy
|
Class |
Drugs |
|
Endothelin antagonists |
Bosentan, Ambrisentan |
|
PDE-5 inhibitors |
Sildenafil, Tadalafil |
|
Prostacyclins |
Epoprostenol, Iloprost |
⚠️ Bosentan can cause hepatotoxicity → monitor LFTs!
🏥 Liver Transplant Considerations
|
Severity |
mPAP |
Implications |
|
Mild |
25–35 mmHg |
Usually acceptable for transplant |
|
Moderate |
35–50 mmHg |
Increased perioperative risk |
|
Severe |
>50 mmHg |
Contraindication to transplant unless optimized with PAH therapy |
📌 PAH therapy → mPAP <35 mmHg → reconsider for transplant
📝 Key Differences: HPS vs. PoPH
|
Feature |
HPS |
PoPH |
|
Pathophysiology |
Vasodilation (NO-mediated) |
Vasoconstriction + remodeling |
|
Pulmonary pressure |
Normal/low |
Elevated (>20 mmHg) |
|
PVR |
Low |
High (>2 WU) |
|
PaO₂ |
Decreased |
Normal/low |
|
Hypoxemia cause |
IPVD/shunt |
↑ PVR → RVF |
|
Treatment |
Liver transplant |
PAH drugs ± transplant |
🔍 Viva/MCQ Pearls
- HPS: Diagnosis via bubble echo
- PoPH: Right heart catheterization is gold standard
- HPS: Orthodeoxia, platypnea
- PoPH: May contraindicate liver transplant
- HPS: ↓ PVR, PoPH: ↑ PVR
- Drug of choice in PoPH: Sildenafil