
Tachy-Brady Syndrome
Definition
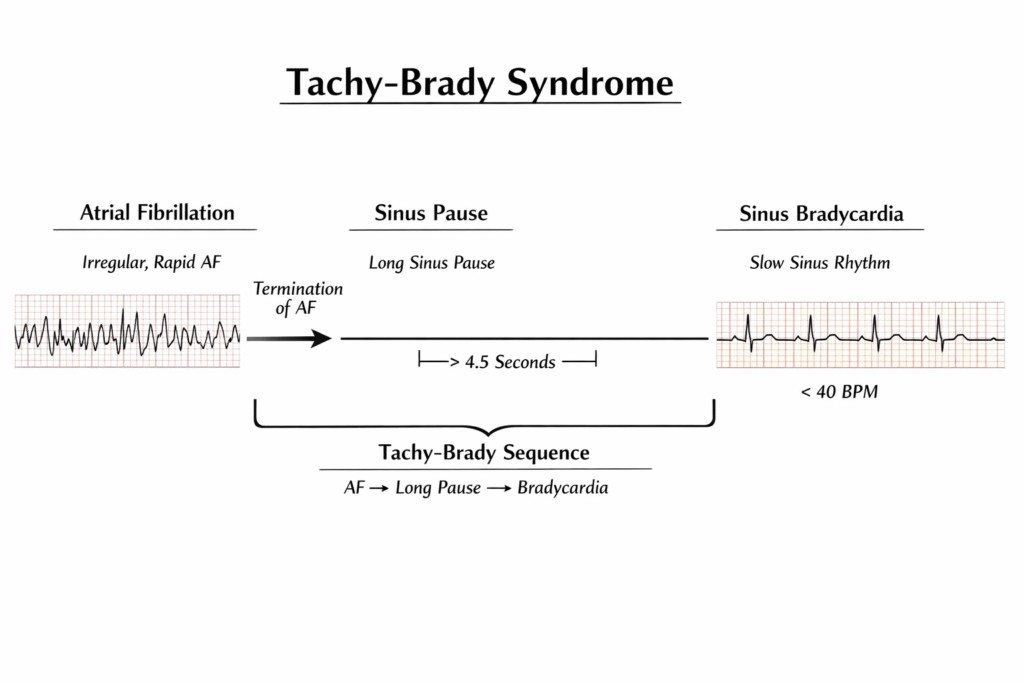
Tachy-Brady Syndrome is a subtype of sinus node dysfunction (SND) in which periods of supraventricular tachyarrhythmia (most commonly atrial fibrillation) alternate with profound sinus bradycardia or sinus pauses, often after termination of the tachyarrhythmia.
It is classically associated with:
- Paroxysmal atrial fibrillation
- Long post-conversion sinus pauses
- Symptomatic bradycardia
Pathophysiology
The condition arises due to degeneration and fibrosis of the sinoatrial (SA) node and surrounding atrial myocardium.
Mechanisms:
- Intrinsic SA node disease
- Age-related fibrosis
- Ischemia (RCA territory infarction)
- Infiltrative disease
- Atrial remodeling
- AF causes electrical remodeling
- Sinus node recovery time becomes prolonged
- Post-tachycardia suppression
- After termination of AF, sinus node fails to resume firing → long pauses
Typical Rhythm Pattern
Phase | Rhythm |
Phase 1 | Atrial fibrillation / atrial flutter |
Phase 2 | Sudden termination |
Phase 3 | Sinus pause (often >3 seconds) |
Phase 4 | Slow sinus rhythm |
Clinical Presentation
Symptoms are due to cerebral hypoperfusion.
Bradycardia Phase:
- Syncope
- Presyncope
- Fatigue
- Dizziness
- Confusion (elderly)
Tachyarrhythmia Phase:
- Palpitations
- Dyspnea
- Chest discomfort
Some patients present with:
- Recurrent syncope
- Stroke (due to AF)
Diagnostic Criteria
Diagnosis requires ECG documentation of both components.
ECG Findings:
- Paroxysmal AF
- Sinus pauses >3 sec
- Sinus bradycardia <50 bpm
- Junctional escape rhythm
Holter Criteria:
- Pauses ≥3 seconds while awake
- Symptomatic bradycardia
- AF followed by long pause
Important:
A pause >5 seconds during sleep may be normal → correlate clinically.
Differential Diagnosis
- AV block
- Carotid sinus hypersensitivity
- Vasovagal syncope
- Drug-induced bradycardia (beta blockers, digoxin, amiodarone)
Management
Acute Management
If unstable:
- Atropine
- Temporary pacing
- Isoproterenol infusion
Definitive Management
1️⃣ Permanent Pacemaker (Cornerstone)
Indications:
- Symptomatic bradycardia
- Documented sinus pauses
- Tachy-brady syndrome requiring rate-control drugs
Usually:
- Dual chamber pacemaker (DDD) preferred
Why?
Because treating AF with beta blockers / amiodarone worsens bradycardia → pacemaker prevents dangerous pauses.
2️⃣ Management of AF Component
After pacemaker placement:
- Beta blockers
- Calcium channel blockers
- Amiodarone (if needed)
- Anticoagulation as per CHA₂DS₂-VASc score
Important Clinical Pearl
Never start aggressive rate-control drugs in suspected tachy-brady syndrome without pacing backup → may precipitate prolonged asystole.