
Sinoatrial Block
What is Sinoatrial (SA) Block?
The SA node generates the impulse normally, but transmission to surrounding atrial tissue is delayed or blocked.
This differentiates it from:
- Sinus bradycardia → slow impulse generation
- Sinus arrest → failure of impulse generation
Anatomy of the SA Node
Location
- Junction of SVC and right atrium
- Subepicardial
Blood Supply
- Right coronary artery (RCA) in ~60%
- Left circumflex artery (LCX) in ~40%
This is clinically important in inferior wall MI, especially right coronary artery infarcts.
Pathophysiology
Impulse generation → SA node
Impulse conduction → Atrial myocardium
In SA block:
- SA node fires normally
- Impulse fails to reach atria
- Result → Dropped P wave + dropped QRS
Mechanism:
- Increased vagal tone
- Ischemia of SA node
- Fibrosis (degenerative disease)
- Drugs
- Electrolyte imbalance
Classification of SA Block
1️⃣ First Degree SA Block
- Delay in conduction from SA node to atrium
- Cannot be diagnosed on surface ECG
- Only detectable via intracardiac recording
Clinically silent.
2️⃣ Second Degree SA Block
Two types:
🔹 Type I (Wenckebach SA Block)
Mechanism
Progressive prolongation of SA conduction until impulse fails.
ECG Features
- Progressive shortening of PP intervals
- Followed by dropped P wave
- Pause less than 2× basic PP interval
Clinical Scenario
- High vagal tone
- Athletes
- Sleep
🔹 Type II SA Block
Mechanism
Sudden failure of conduction without prior PP change.
ECG Features
- Constant PP intervals
- Sudden dropped P wave
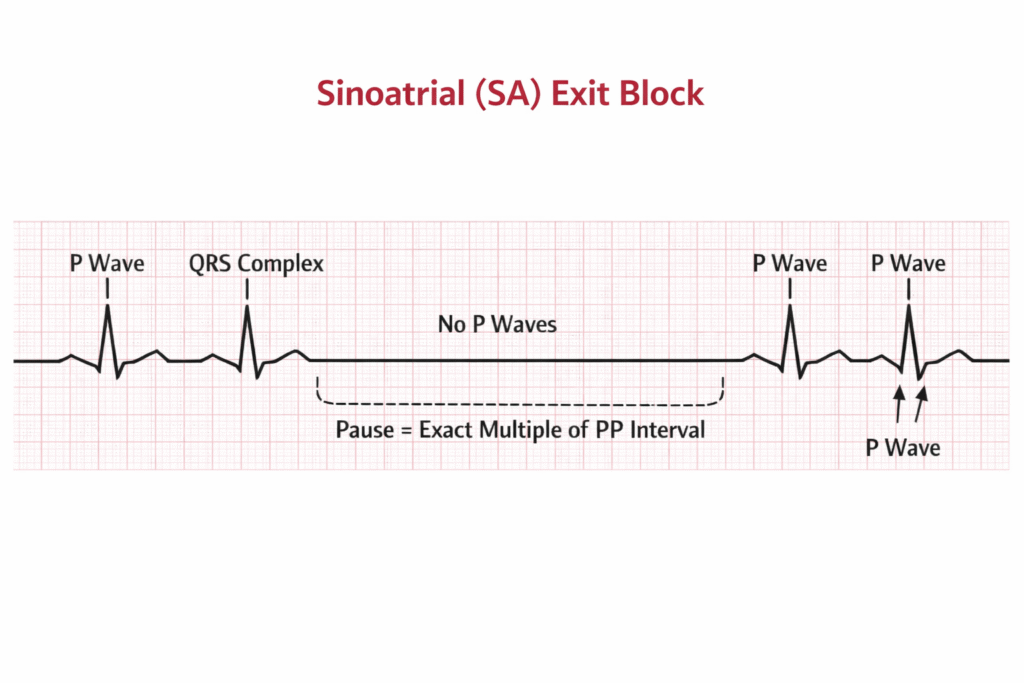
- Pause = multiple of basic PP interval (e.g., 2×, 3×)
More dangerous than Type I
Associated with:
- SA node ischemia
- Fibrosis
- Sick sinus syndrome
3️⃣ Third Degree SA Block (Complete SA Block)
- No impulses conducted to atria
- Atrial standstill
- Escape rhythm appears (junctional or ventricular)
ECG:
- No P waves
- Escape rhythm present
This resembles sinus arrest but differs mechanistically.
Feature | Third-Degree SA Block | Sinus Pause / Arrest |
Mechanism | Exit block | Failure of impulse generation |
Pause duration | Exact multiple of basic PP interval | Not a multiple of PP interval |
Predictability | Regular timing | Irregular |
Underlying PP cycle | Maintained internally | Disrupted |
Escape rhythm | Usually present | May or may not appear |
ECG Patterns
Etiology of SA Block
1️⃣ Increased Vagal Tone
- Athletes
- Sleep
- Carotid sinus stimulation
2️⃣ Ischemia
- Inferior wall MI (RCA)
- Right ventricular infarction
3️⃣ Degenerative Fibrosis
- Elderly
- Sick sinus syndrome
4️⃣ Drugs
- Beta blockers
- Calcium channel blockers
- Digoxin
- Amiodarone
5️⃣ Electrolyte Disturbances
- Hyperkalemia
6️⃣ Infiltrative Disease
- Amyloidosis
- Sarcoidosis
Clinical Presentation
Asymptomatic (most common)
Symptomatic
- Dizziness
- Presyncope
- Syncope
- Fatigue
- Exercise intolerance
Severe cases → Stokes–Adams attacks
Hemodynamic Consequences
- Reduced cardiac output
- Loss of atrial kick
- Hypotension
- Worsened in elderly / LV dysfunction
Diagnosis
1️⃣ ECG
Primary tool.
2️⃣ Holter Monitoring
Useful for intermittent episodes.
3️⃣ Electrophysiology Study
Rarely needed.
Permanent Pacemaker
Indications:
- Symptomatic bradycardia
- Documented pauses >3 seconds with symptoms
- Sick sinus syndrome
Preferred mode:
- Dual chamber pacing (DDD)