
Sinus Node Dysfunction
1. Introduction
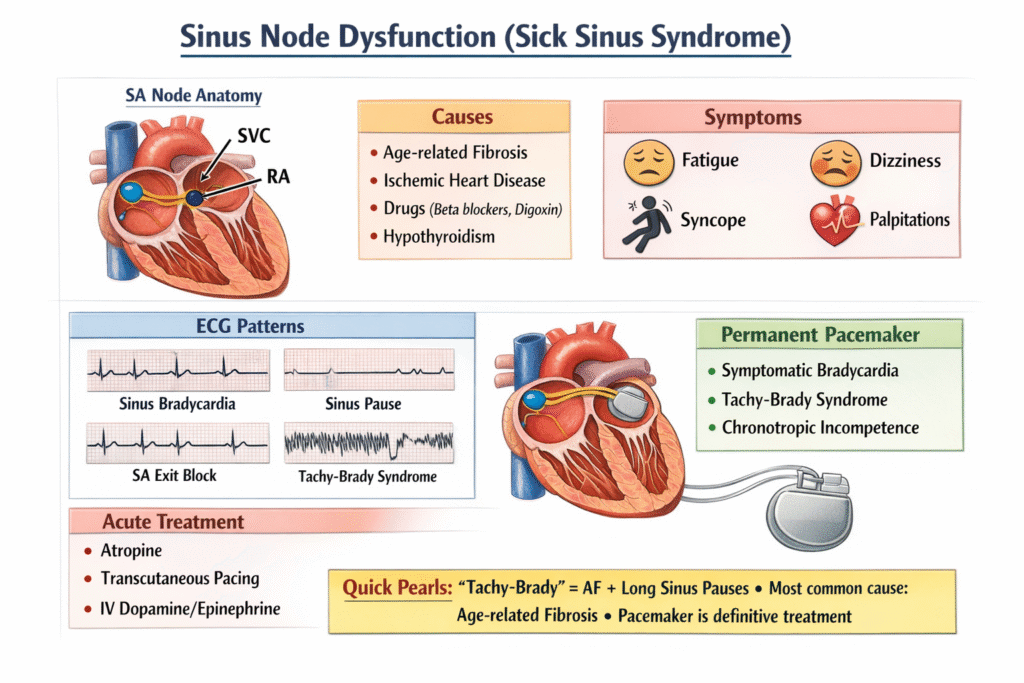
Sinus Node Dysfunction (SND) refers to a spectrum of disorders caused by abnormal impulse generation and propagation from the sinoatrial (SA) node, leading to symptomatic bradyarrhythmias.
Also known as:
- Sick Sinus Syndrome (SSS)
- Sinus Node Disease
- Tachy-brady Syndrome (when AF alternates with bradycardia)
Sinus Node Dysfunction is defined as:
Inappropriate sinus bradycardia, sinus pauses, sinus arrest, or sinoatrial block causing symptoms due to impaired SA node automaticity or conduction.
2. Anatomy & Physiology
Location
- Located in high right atrium, near the junction of SVC and RA
Blood Supply
- SA nodal artery from:
- RCA (≈60%)
- LCx (≈40%)
Hence → Inferior MI (RCA territory) can cause transient SND.
Electrophysiology
Automaticity via:
- Funny current (If)
- Calcium-dependent depolarization
- Autonomic modulation
Normal intrinsic rate: 90–110 bpm
Resting rate is lower due to vagal tone
3. Epidemiology
- Most common in elderly (>65 years)
- Age-related fibrosis is major cause
- Increasing incidence due to aging population
- One of the leading causes of pacemaker implantation
4.Etiology
A. Intrinsic Causes (Structural SA Node Disease)
- Age-related fibrosis (most common)
- Ischemic heart disease (especially inferior MI)
- Infiltrative diseases:
- Amyloidosis
- Sarcoidosis
- Hemochromatosis
- Post-cardiac surgery
- Congenital SND (rare)
- Genetic ion channel mutations (HCN4 mutation)
B. Extrinsic (Reversible) Causes
✔ Always rule out before labeling SND
- Drugs:
- Beta blockers
- Non-DHP CCBs
- Digoxin
- Amiodarone
- Clonidine
- Hypothyroidism
- Hyperkalemia
- Hypoxia
- Increased vagal tone
- Sleep apnea
- Raised ICP
5. Clinical Manifestations
Symptoms due to:
- Low cardiac output
- Cerebral hypoperfusion
- Pause-dependent ventricular arrhythmias
Common Symptoms:
- Fatigue
- Dizziness
- Syncope
- Presyncope
- Exercise intolerance
- Palpitations (if tachy-brady)
- Heart failure exacerbation
⚠️ Many patients are asymptomatic.
6. ECG Patterns in SND
1️⃣ Sinus Bradycardia
- HR < 50 bpm (inappropriately low)
2️⃣ Sinus Pause
- Pause > 2–3 seconds
3️⃣ Sinus Arrest
- No P wave
- Pause not multiple of P-P interval
4️⃣ SA Exit Block
- Pause is multiple of P-P interval
5️⃣ Tachy-Brady Syndrome
- AF alternating with long pauses
7. Diagnostic Criteria
Diagnosis requires:
✔ Symptoms attributable to bradycardia
✔ ECG documentation
Tools:
- 12-lead ECG
- Holter (24–48 hr)
- Event recorder
- Implantable loop recorder (if unexplained syncope)
8. Differential Diagnosis
- AV block
- Carotid sinus hypersensitivity
- Vasovagal syncope
- Drug-induced bradycardia
- Hypothyroidism
9. Acute Management (ICU Approach)
If symptomatic bradycardia:
According to ACLS protocol:
- Atropine 1 mg IV (repeat q3–5 min; max 3 mg)
- If ineffective:
- Transcutaneous pacing
- Dopamine infusion
- Epinephrine infusion
Atropine may be less effective in intrinsic SND.
10. Indications for Permanent Pacemaker
Permanent pacing is the definitive treatment.
Class I Indications (Strong Recommendation)
- Symptomatic sinus bradycardia
- Symptomatic sinus pauses
- Tachy-brady syndrome with symptoms
- Chronotropic incompetence with symptoms
NOT Indicated:
- Asymptomatic bradycardia
- Physiologic bradycardia (athletes)
- No documented correlation with symptoms
11. Type of Pacemaker
Preferred: Dual chamber (DDD)
Why?
- Maintains AV synchrony
- Reduces AF risk
- Reduces stroke risk
- Prevents pacemaker syndrome
Single chamber (AAI) rarely used.
12. Chronotropic Incompetence
Definition:
Failure to increase heart rate appropriately during exercise.
Diagnosed by:
- Exercise stress test
- Failure to achieve 80% age-predicted HR reserve
Common cause of exertional fatigue.
13. Special Situations
SND in Acute MI
- Usually inferior MI
- Often transient
- Observe unless persistent
Sleep Apnea
Treat OSA before pacemaker decision.
Drug-Induced SND
Stop offending agent first.
14. Complications of Untreated SND
- Recurrent syncope
- Falls
- Heart failure
- Stroke (if AF present)
- Sudden cardiac death (rare)