
Subarachnoid Hemorrhage (SAH)
Subarachnoid hemorrhage (SAH) is bleeding into the subarachnoid space between the arachnoid mater and pia mater where cerebrospinal fluid (CSF) circulates.
It is one of the most devastating neurological emergencies with:
- Mortality: 25–50%
- Significant disability among survivors
- Peak incidence: 40–60 years
Approximately 80–85% of spontaneous SAH results from rupture of an intracranial aneurysm.
Table of Contents
ToggleRelevant Anatomy
The subarachnoid space contains:
- Cerebral arteries
- Cerebral veins
- Cranial nerves
- CSF
Blood entering this space spreads rapidly throughout basal cisterns and ventricular system causing:
- Raised ICP
- Cerebral ischemia
- Hydrocephalus
- Vasospasm
Etiology
Aneurysmal SAH (Most Common)-80–85%
Common aneurysm locations:
Anterior circulation (85%)
- Anterior communicating artery (ACom) (most common)
- Posterior communicating artery (PCom)
- Middle cerebral artery (MCA)
Posterior circulation
- Basilar tip
- Vertebral artery
- PICA
Non-Aneurysmal SAH
Perimesencephalic SAH
- Venous bleeding
- Better prognosis
- Rare rebleeding
Others
- AVM rupture
- Dural AV fistula
- Vasculitis
- Cerebral venous thrombosis
- Moyamoya disease
- Coagulopathy
- Cocaine abuse
- Trauma
Risk Factors
Nonmodifiable Risk Factors | Modifiable Risk Factors |
Female sex | Hypertension – Most important risk factor |
Age >40 years | Smoking – Strongest modifiable risk factor |
Family history | Alcohol – Heavy consumption increases risk |
Connective tissue disorders | Cocaine use – Markedly increases aneurysm rupture risk |
• Ehlers-Danlos syndrome |
|
• Marfan syndrome |
|
• Autosomal Dominant Polycystic Kidney Disease (ADPKD) |
|
Pathophysiology
Step 1: Aneurysm Rupture
Arterial blood suddenly enters subarachnoid space.
Step 2: Sudden ICP Rise
ICP may transiently approach MAP.
Consequences:↓ Cerebral perfusion pressure
CPP=MAP−ICP
This produces:
- Global cerebral ischemia
- Loss of consciousness
- Cardiac instability
Step 3: Blood Breakdown Products
Hemoglobin degradation releases:
- Oxyhemoglobin
- Free radicals
- Endothelin
Leading to:
- Endothelial injury
- Vasoconstriction
- Inflammation
Step 4: Delayed Cerebral Ischemia
Occurs days later.
Major cause of morbidity.
Step 5: Hydrocephalus
Blood blocks:
- Arachnoid granulations
- CSF pathways
Result:Acute obstructive hydrocephalus.
Clinical Presentation
- Thunderclap Headache(usually defined as a severe headache that peaks in <1 minute)
- Patient often says:”Worst headache of my life”
Characteristics:
- Abrupt
- Seconds to minutes
- Explosive onset
Occurs in >90%.neither sensitive nor specific.
Associated Symptoms
Meningeal Irritation
- Neck stiffness
- Photophobia
- Vomiting
Neurological Symptoms
- Altered sensorium
- Seizures
- Focal deficits
- Coma
Cranial Nerve Palsies
CN III palsy-Suggests PCom aneurysm.
Features:
- Ptosis
- Dilated pupil
- Ophthalmoplegia
CN-6 palsy may result from elevated intracranial pressure.
Sentinel Headache
- Occurs days to weeks before rupture.
- Represents minor aneurysm leak.
- Seen in 10–40%.
Physical Examination
Vital Signs
May show:
- Severe hypertension
- Bradycardia
- Cushing response
Neurological Findings
- Meningismus
- Reduced GCS
- Focal deficits
- Coma
Diagnosis
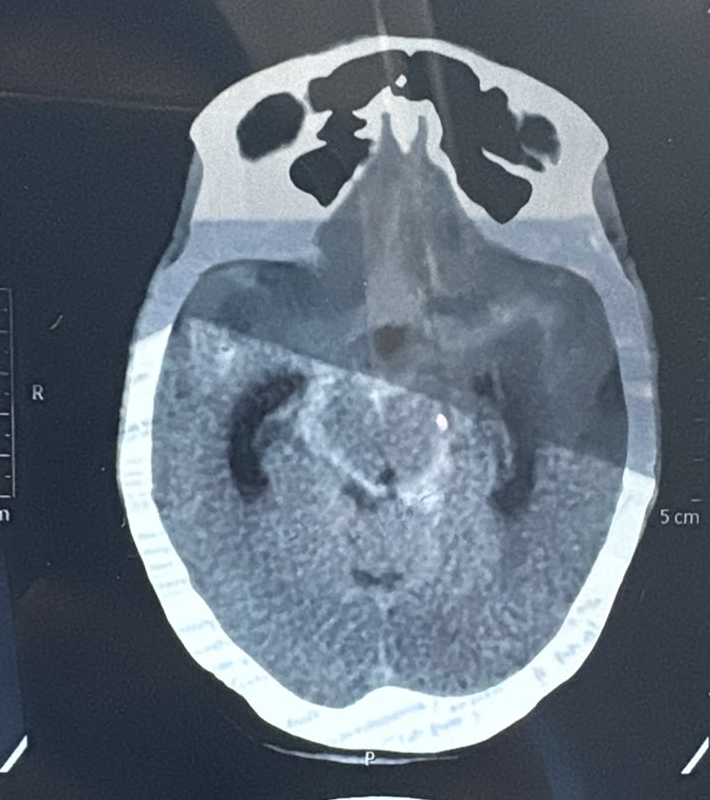
Non-Contrast CT Head-First-line investigation.If NCCT confirms SAH, the next step is usually vascular imaging (CTA or DSA) to identify the bleeding source.
Time | Sensitivity |
<6 h | >95–99% |
6–24 h | 90–95% |
>3 days | Falls significantly |
Typical findings:
- Basal cistern blood
- Sylvian fissure blood
- Intraventricular hemorrhage
- Hydrocephalus
Lumbar Puncture
- Indication:High suspicion despite negative CT.(primarily if the CT scan was obtained >6 hours after headache onset)
- Look for:Xanthochromia(yellow hue observed in CSF due to RBC breakdown)
- Best detected:12 hours–2 weeks
- Findings:
- Bilirubin in CSF
- Persistent RBCs
- Falling RBC counts from tube #1 to tube #4 can be seen with both a traumatic tap and a SAH therefore could not differentiate between the two.in this case xanthocromia will help
CT Angiography (CTA)
CTA is not recommended in every patient with SAH automatically, but it is recommended in most patients once SAH is diagnosed or strongly suspected, particularly to identify a ruptured aneurysm and guide treatment.
Identifies:
- Aneurysm
- AVM-arteriovenous malformations).
- Vasospasm
- Reversible Cerebral Vasoconstriction Syndrome (RCVS) or cervical artery dissection.
Sensitivity >95%.Very small aneurysms may be missed
Digital Subtraction Angiography (DSA)
Gold standard.
Used when:
- CTA negative
- High suspicion remains
- Endovascular planning
- Perimesencephalic SAH pattern with uncertain source
The initial angiogram may occasionally be negative due to vasospasm or local thrombosis, which prevents contrast from entering the aneurysm.
MRI
- Useful later.
- FLAIR(acute phase of SAH, showing sulcal hyperintensity.)
- GRE—SWI(detect hemosiderin )
- Less useful in hyperacute setting.
- For patients with SAH near the base of the brain and no defined source of bleeding, cervical spine MRI may be useful to evaluate for a spinal source of bleeding.
Severity Grading
Hunt & Hess Scale | WFNS Grade (Based on GCS) | Modified Fisher Scale |
Grade I – Asymptomatic or mild headache, slight nuchal rigidity. | Grade I – GCS 15, no focal neurological deficit. | Grade 0 – No SAH or IVH. |
Grade II – Moderate to severe headache, nuchal rigidity, cranial nerve palsy may be present. | Grade II – GCS 13–14, no focal neurological deficit. | Grade 1 – Thin SAH (<1 mm), no IVH. |
Grade III – Drowsiness, confusion, mild focal neurological deficit. | Grade III – GCS 13–14 with focal neurological deficit. | Grade 2 – Thin SAH (<1 mm) with IVH. |
Grade IV – Stupor, moderate-to-severe hemiparesis, early decerebrate rigidity, autonomic disturbances. | Grade IV – GCS 7–12, with or without focal deficit. | Grade 3 – Thick SAH (≥1 mm), no IVH. |
Grade V – Deep coma, decerebrate posturing, moribund appearance. | Grade V – GCS 3–6, with or without focal deficit. | Grade 4 – Thick SAH (≥1 mm) with IVH. |
Predicts: Mortality, functional outcome, perioperative risk. | Predicts: Outcome; has better interobserver reliability than Hunt–Hess. | Predicts: Risk of vasospasm and delayed cerebral ischemia (DCI). |
Limitation: Subjective and examiner-dependent. | Advantage: More objective due to GCS-based classification. | Most commonly used CT grading system today. |
Current Role: Historically important; still widely reported in studies. | Current Role: Preferred clinical grading system in modern SAH literature and guidelines. | Current Role: Preferred radiological grading system for vasospasm/DCI risk stratification. |
Emergency Stabilization
ABC Approach
Blood Pressure Management
- Before Aneurysm Securing Major goal:Prevent rebleeding.
- SBP Target:120–160 mmHg(AHA 2023 guidelines don’t specify any target).Target at patient’s baseline.
Preferred Antihypertensives
Drug | Comment |
Nicardipine infusion | Most commonly used |
Clevidipine infusion | Excellent titratable agent |
Labetalol bolus/infusion | Commonly used |
Esmolol | Occasionally used |
Avoid:
Drug | Reason |
Nitroprusside | May increase ICP |
Nitroglycerin | May increase ICP |
Hydralazine | Unpredictable effect |
Definitive Aneurysm Treatment
Should occur as early as possible (usually within 24 h).
Blood pressure target(e.g.SBP <200 mm).
Endovascular Coiling
Current preferred approach in many aneurysms.
Advantages:
- Less invasive
- Better short-term outcomes
Surgical Clipping
Preferred when:
- MCA aneurysm
- Large hematoma
- Complex anatomy
Tranexamic Acid
ULTRA trial showed that ultra-early (<24 h), short-course TXA reduces rebleeding tendency but does not improve 6-month functional outcome in aneurysmal SAH; therefore routine TXA use is not recommended.
Pharmacologic DVT Prophylaxis
=Before Aneurysm Securing
- Withheld until aneurysm is secured.
- Reason:Potential risk of catastrophic rebleeding.
=After Coiling or Clipping
Once:
- Aneurysm secured
- Repeat imaging stable after >24 hours
- Neurosurgical approval obtained
Then start:
Drug | Dose |
Enoxaparin(Preferred because less risk of Heparin-induced thrombocytopenia ) | 40 mg SC daily |
UFH | 5000 U SC q8–12h |
IF EVD Present?
Pharmacologic prophylaxis can still be used
After:
- Stable CT
- Neurosurgical agreement
Temporary withholding around EVD insertion/removal is common.
Coagulopathy Management
- Target Platelet->1lakh
- Target INR<1.4
- Avoid NSAID for pain.
Reversal of medications:
- Warfarin reversal
- Dabigatran reversal
- Xaban reversal
- Thrombolysis reversal
- Heparin reversal
- Antiplatelet reversal: (DDAVP may be considered:)
Anemia and Transfusion Targets
The 2023 AHA/ASA SAH guideline acknowledges that anemia is associated with poor outcomes but concludes that evidence is insufficient to recommend a specific transfusion threshold for all patients with aSAH.
Therefore:
❌ No guideline-mandated Hb target exists.
❌ No recommendation to routinely maintain Hb >10 g/dL.
❌ No recommendation to use standard ICU thresholds (Hb <7 g/dL) in all SAH patients.
- Transfusion decisions should be individualized based on neurological status, DCI risk, and overall clinical condition.
- hemoglobin level of >9 mg/dL may be beneficial(TRAIN trial)
SAHARA Trial (NEJM 2025)
- Liberal Strategy(Transfuse when Hb ≤10 g/dL) vs Restrictive Strategy(Transfuse when Hb ≤8 g/dL)
- A liberal transfusion strategy did not improve 12-month neurological outcomes compared with a restrictive strategy.
Analgesia
- Headache is one of the most prominent symptoms of SAH and may persist for days to weeks due to ongoing meningeal irritation from blood products within the subarachnoid space.
- Effective pain control is important not only for patient comfort but also to prevent sympathetic activation, hypertension, agitation, and increased intracranial pressure.
General Principles
- Adequate analgesia should be provided while preserving the ability to perform reliable neurological examinations.
- Excessive sedation should be avoided because it may mask neurological deterioration.
Analgesic Options
1. Acetaminophen (Paracetamol)
- Often considered first-line therapy.
- Can be administered on a scheduled basis (e.g., 1 g every 6 hours, maximum daily dose adjusted for liver function and body weight).
2. Gabapentin
- Typical dosing ranges from 300–900 mg three times daily, titrated according to renal function and tolerability.
3. Migraine-Directed Therapies
Many SAH headaches share features with severe migraine and may respond to:
- Metoclopramide
- Prochlorperazine
- Intravenous magnesium sulfate
These agents can be particularly useful when headache is accompanied by nausea, vomiting, or photophobia.
4. Valproic Acid
- May be considered for refractory headache.
- A commonly used regimen is 500 mg IV over 15 minutes.
- Limited evidence suggests potential benefit in patients with persistent severe headache despite conventional therapy.
5. Opioids
- Should be used cautiously and preferably as intermittent PRN doses for breakthrough pain.
Additional Measures Often Overlooked
- Treat associated nausea and vomiting aggressively.
- Minimize environmental triggers (noise, bright light).
- Control fever, which may exacerbate headache and neurological injury.
- Address hydrocephalus, vasospasm, or elevated intracranial pressure if headache worsens unexpectedly despite analgesia.
Fever Management
- Fever is a common complication after aneurysmal SAH, occurring in 40–70% of patients.
- Central (Neurogenic) Fever is a noninfectious fever caused by hypothalamic dysfunction and neuroinflammation following brain injury.
- Central fever is a diagnosis of exclusion.
- Before labeling a fever as neurogenic, infectious causes must be reasonably excluded.(Blood cultures,Sputum Gram stain and culture,Urine culture,CSF (if EVD present).Although none are diagnostic, central fever is more likely when:Poor response to antibiotics,Intraventricular hemorrhage,Early onset (within first 72 hours)
Treatment of Fever
1. Antipyretic Therapy (First-Line)
Acetaminophen (Paracetamol)
- Usually first-line treatment.
- 1 g every 6 hours
- Adjust for hepatic dysfunction.
2. Physical Cooling
- Cooling blankets/Surface cooling pads
- Adaptive external cooling systems/Endovascular cooling devices
Advantages
- More effective temperature reduction.
- Faster achievement of normothermia.
Disadvantages—Shivering
Management of Shivering
Shivering can negate many benefits of cooling.
Common anti-shivering strategies:
Nonpharmacologic
- Counterwarming of hands and feet
- Warm blankets
Pharmacologic
- Acetaminophen
- Magnesium infusion
- Buspirone
- Meperidine (pethidine)
- Dexmedetomidine
- Propofol (selected patients)
Bromocriptine
Dopamine agonist that may modulate hypothalamic thermoregulation.
Evidence
- Limited to case reports and small case series.
- No high-quality randomized trials.
Role
May be considered in:
- Suspected central fever
- Persistent fever despite antipyretics
- Failure of conventional therapy
Typical reported doses:
- 2.5–10 mg orally every 6–8 hours
However, evidence remains limited.
ICU Monitoring
Daily assessment:
- Neurological examination
- GCS
- Pupils
- TCD
- Electrolytes
- Fluid balance
ICU Targets
Parameter | Target |
SpO₂ | >94% |
PaO₂ | >80 mmHg |
Temperature | Normothermia |
Glucose | 140–180 mg/dL |
Sodium | Normal range |
CPP | >60–70 mmHg |
ICP | <20–22 mmHg |
Rebleeding
Highest Risk Period-First 24 hours.
Clinical Features
- Neuroworsening occurs (e.g., new obtundation/coma, extensor posturing, loss of cranial nerve reflexes).
- headache and vomiting .
- Signs of Raised ICP .
- fresh blood from a ventriculostomy drain.
Prevention
- Early coiling/clipping
- BP control
- Avoid agitation
Delayed Cerebral Ischemia (DCI)
- Most important delayed complication.
- Occurs:Day 4–14
- Peak:Day 7–10
- Resolved by day 21
Mechanism
Not solely vasospasm.
Also:
- Microthrombosis
- Inflammation
- Cortical spreading depolarization
Clinical Features
New:
- Weakness
- Aphasia
- Reduced consciousness
Diagnosis
- TCD-Mean MCA velocity:
- 120 cm/s suggests vasospasm
- 200 cm/s severe vasospasm
- Lindegaard ratio >3–6.
- cEEG –may predict vasospasm up to 3 days before its onset
- CTA-Useful screening tool.
- CT perfusion—providing information about tissue perfusion
- MRI—shows areas of ischemic tissue could support a diagnosis of symptomatic vasospasm.
- DSA(invasive angiography)-Gold standard.
Prevention of Vasospasm—
Nimodipine
- Dose-60 mg orally/NG every 4 h
- Duration:-21 days
- If hypotension:-30 mg every 2h.
- Give to all aneurysmal SAH patients unless contraindicated.
Euvolemia
Eumagnesemia
Treatment of Symptomatic Vasospasm/DCI
- Optimize:Oxygenation/Hemoglobin/Volume status/hypomagnesemia
- Induced Hypertension Recommended for symptomatic DCI after aneurysm securing.Elevate MAP by ~20 mm above baseline.elevated MAP may be maintained for 2-3 days, after which augmentation is cautiously weaned over several days. .Contraindications:
- Neurogenic stunned myocardium.
- Cardiac failure/cardiogenic shock.
- Severe baseline hypertension (pushing the MAP too high may cause PRES).
- Aneurysm remains unsecured.
Common Targets
Severity | SBP Target |
Mild DCI | 160–180 mmHg |
Moderate DCI | 180–200 mmHg |
Severe DCI | Up to 220 mmHg in selected patients |
or
Parameter | Target |
MAP | 90–130 mmHg |
Targets are individualized.
Vasopressors Used
Drug | Preferred? |
Norepinephrine | Yes |
Phenylephrine | Yes |
Vasopressin | Occasionally |
Dopamine | Rarely |
- Endovascular Therapy-Balloon angioplasty.Best for proximal vessels.
- Intra-arterial vasodilators—Verapamil,Nicardipine
- I.V Milrinone(0.5 ug/kg/min)
Triple-H Therapy
Historical:
- Hypertension
- Hypervolemia
- Hemodilution
No longer recommended.
Current practice:Euvolemia + induced hypertension only.
Hydrocephalus
Occurs in 15–30%.
Features:
- Reduced consciousness
- Enlarged ventricles
- ICP elevation
- The best predictor of hydrocephalus is a poor clinical grade of SAH.
Treatment—External Ventricular Drain (EVD)
—Lumbar Drain(contraindicated in obstructive hydrocephalus )
Provides:
- CSF diversion
- ICP monitoring
Current Practice
- Periprocedural antibiotic prophylaxis commonly used
- Prolonged antibiotics for entire EVD duration are not recommended
Typical example:
- Cefazolin before insertion
Extended prophylaxis has not shown benefit and increases resistant organisms.
ICP Management
Treat when:ICP >20–22 mmHg
Measures:
- Head elevation 30°
- Sedation
- Analgesia
- CSF drainage(Elevated ICP may persist even after placement of an external ventricular drain.)
- Hyperosmolar therapy
Hypertonic Saline
Preferred in many ICUs.
Mannitol
0.25–1 g/kg
Useful when:
- ICP crisis
- Hemodynamic stability
Seizures
Incidence:6–20%
Risk factors:
- Cortical hematoma
- MCA aneurysm
- Rebleeding
- Hydrocephalus
- intraparenchymal hemorrhage
Antiepileptic Therapy
- Not routinely given long-term.
- Short-course prophylaxis ~3-7 days may be used in:High-risk patients,prophylaxis can be discontinued after seizure has been excluded (either via EEG or clinical examination), and the aneurysm has been secured.
- Common agents:
- Levetiracetam(preferred,Augmented renal clearance should be considered.)
- Valproate
- Phenytoin not recommended
Classification
Timing | Definition | Significance | ASM Duration |
Onset seizure | At rupture/presentation | Acute cortical irritation caused by subarachnoid blood. | ≤7 days often sufficient |
Early seizure(Acute symptomatic seizure) | 0–7 days |
| Usually >7 days depending on risk factors |
Late in-hospital seizure | 7–14 days | Often associated with DCI/infarction | Usually extended therapy |
Post-SAH epilepsy | >14 days or post-discharge | Unprovoked seizure disorder | Long-term ASM |
Continuous EEG (cEEG): An Often-Missed Point
Indications
Continuous EEG should be strongly considered in:
- Persistent unexplained depressed consciousness.
- Failure to awaken after aneurysm treatment.
- Suspected non-convulsive seizures.
- Suspected non-convulsive status epilepticus.
- Fluctuating neurological examination.
Sodium Disorders
Very common.
- SIADH(Because hypovolemia can precipitate vasospasm, fluid restriction or diuretics should be avoided, use 3% N.S)
- Cerebral Salt Wasting
- Pseudohyponatremia (due to mannitol)
- Adrenal insufficiency due to hypothalamic/pituitary axis dysfunction.
Cardiac Complications
Due to catecholamine surge.
-ECG Changes
- QT prolongation
- ST changes
- T-wave inversion
-Arrhythmias—AF/VT/Bradycardia
-Stress/takotsubo Cardiomyopathy
- Neurogenic stunned myocardium.
- Can mimic MI.
Pulmonary Complications
- Neurogenic pulmonary edema
- ARDS
- Aspiration pneumonia
- Cardiogenic pulmonary edema primarily due to takotsubo cardiomyopathy
- Iatrogenic volume overload.
Clinical Notes
- ACom aneurysm = most common aneurysm causing SAH.
- Thunderclap headache = hallmark presentation.
- Non-contrast CT is first investigation.
- Negative CT + high suspicion → LP for xanthochromia.
- DSA = gold standard vascular study.
- Rebleeding risk highest during first 24 hours.
- Nimodipine is the only drug proven to improve neurological outcome.
- Vasospasm typically occurs day 3–14, peaks day 7.
- DCI is now considered more important than angiographic vasospasm alone.
- Triple-H therapy is obsolete.
- EVD is treatment of acute hydrocephalus.
- Induced hypertension is used for symptomatic DCI after aneurysm securing.
- Hyponatremia after SAH is commonly due to SIADH or cerebral salt wasting.
- Neurogenic stunned myocardium is a classic extracranial complication.
- Early aneurysm coiling/clipping is the single most important intervention to prevent rebleeding.