
Ventilator Asynchronies
Ventilator asynchrony refers to a mismatch between the patient’s neural respiratory drive and the ventilator’s delivered breath (trigger, flow, cycling, or mode).
It leads to:
- ↑ Work of breathing (WOB)
- Patient discomfort
- Sedation escalation
- Delirium
- Prolonged mechanical ventilation
- Increased ICU stay
- Possibly increased mortality
Asynchrony is present in up to 20–40% of ventilated ICU patients, and severe asynchrony index (>10%) is associated with worse outcomes.
Table of Contents
ToggleClassification of Ventilator Asynchronies
Ventilator asynchronies are classified according to the phase of the breath cycle:
Phase | Type of Asynchrony |
Trigger phase | Trigger delay, ineffective trigger, auto-triggering |
Inspiratory phase | Flow starvation (flow mismatch),Excessive flow |
Cycling phase | Premature cycling, delayed cycling |
Breath delivery | Double triggering, breath stacking |
Mode-related | Reverse triggering |
Asynchrony Index (AI)
AI=Number of asynchronous events/Total respiratory rate ×100
Where:Total respiratory rate = ventilator breaths + ineffective efforts
AI | Interpretation |
<10% | Acceptable |
>10% | Significant asynchrony |
>20% | Severe asynchrony |
AI >10% has been associated with prolonged ventilation and worse outcomes.

Ineffective Triggering (Missed Trigger)Definition: Patient effort fails to trigger ventilator breath. Causes:
| Pressure waveform:Small negative deflection not followed by a breath. Flow waveform:Small inspiratory dip without breath delivery. Most common ventilator asynchrony. |
|
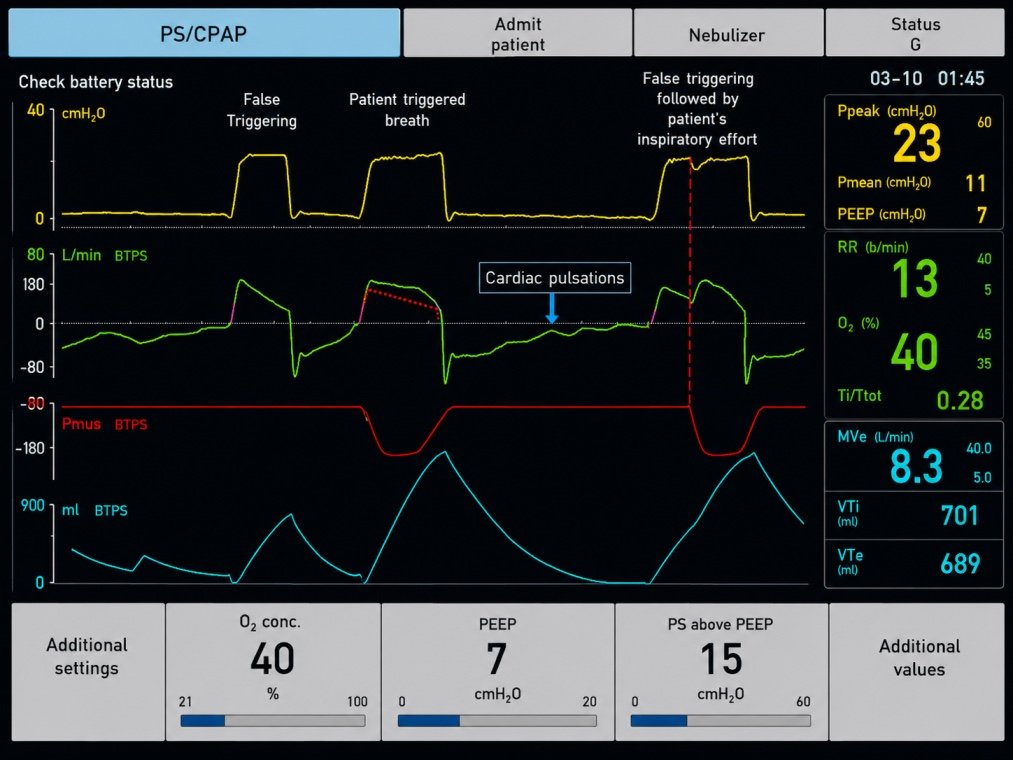
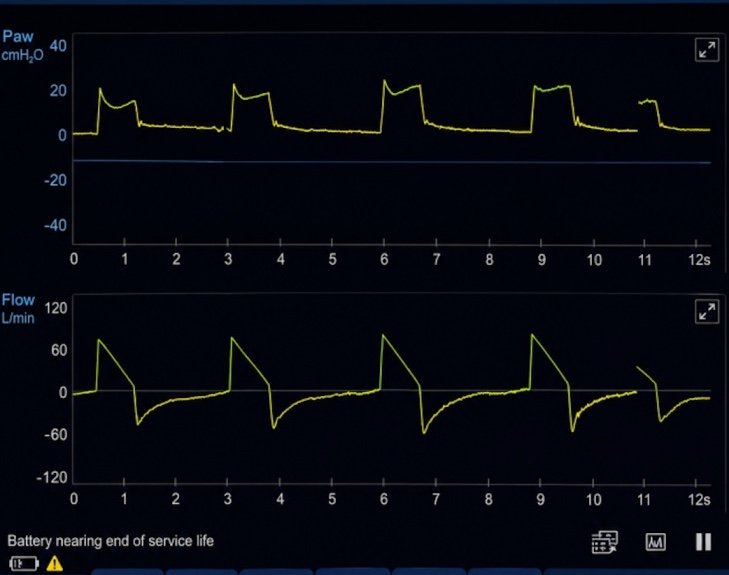
Auto-Triggering Definition: Ventilator delivers breaths without patient effort. Causes:
| Breaths occur without pressure deflection, inspiratory effort, or diaphragmatic activity. Respiratory rate appears higher than actual patient effort. |
|

Double Triggering Definition: One inspiratory effort triggers two consecutive breaths separated by minimal expiratory time. Causes:
| Two consecutive breaths with little or no exhalation between them (“breath stacking”). May result in excessive tidal volume. |
|
Reverse TriggeringDefinition: Ventilator breath induces diaphragmatic contraction (patient follows ventilator). Causes:
Patterns: 1:1 or 1:2 entrainment. |
Patient effort begins aftermachine breath starts. Regular entrainment pattern (1:1 or 1:2). May cause breath stacking and high transpulmonary pressures. |
|
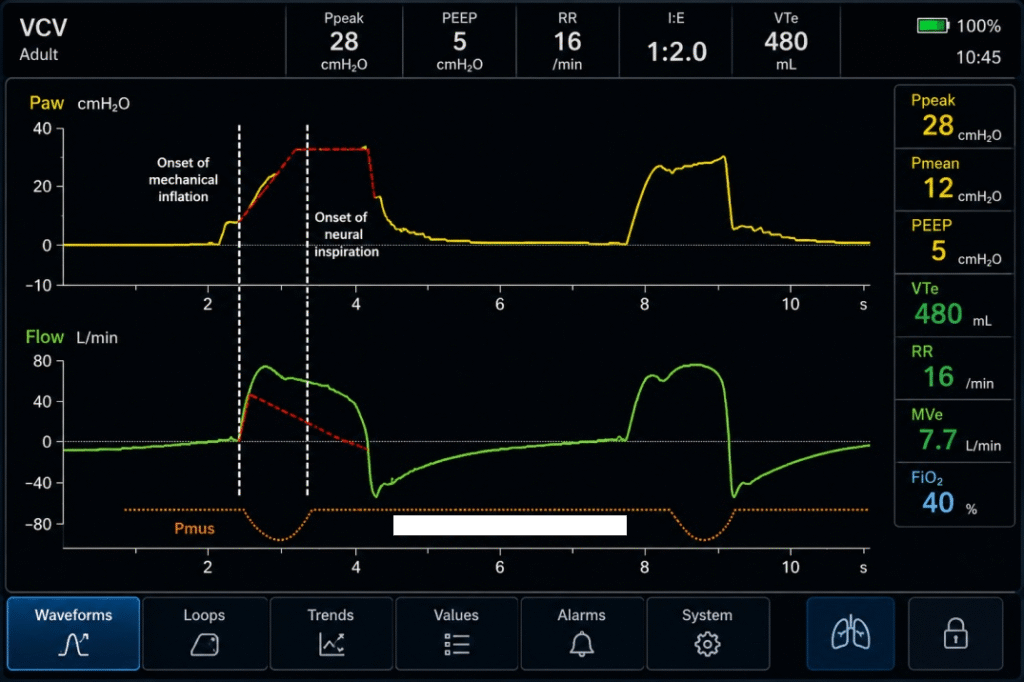
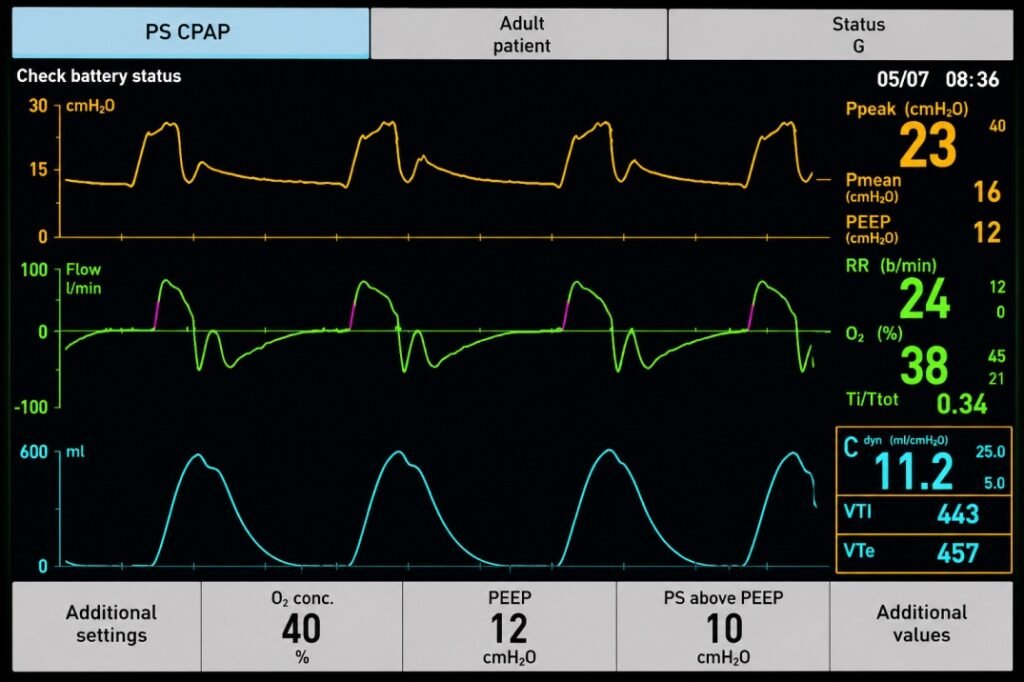
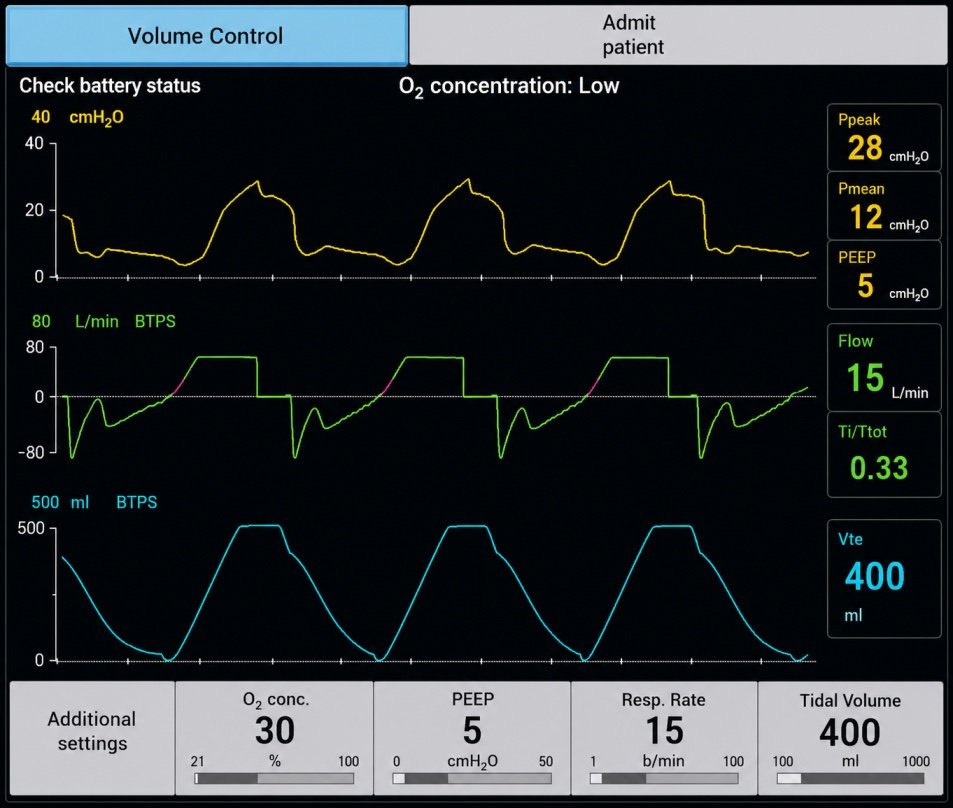
Flow StarvationDefinition: Ventilator delivers less inspiratory flow than the patient demands. Most common in:Volume-Control Ventilation (VCV). Causes:
| Pressure-time waveform:Characteristic “scooped” or concave downward appearance during inspiration due to patient pulling additional flow. inspiratory pressure curve dips inward (“fish-hook” appearance).
|
|
Excessive Flow (Flow Overshoot)Definition: Ventilator delivers inspiratory flow faster than the patient desires. Causes:
| Pressure-time waveform: Early inspiratory pressure spike (“overshoot”) followed by stabilization. Patient may actively exhale during inspiration.
|
|
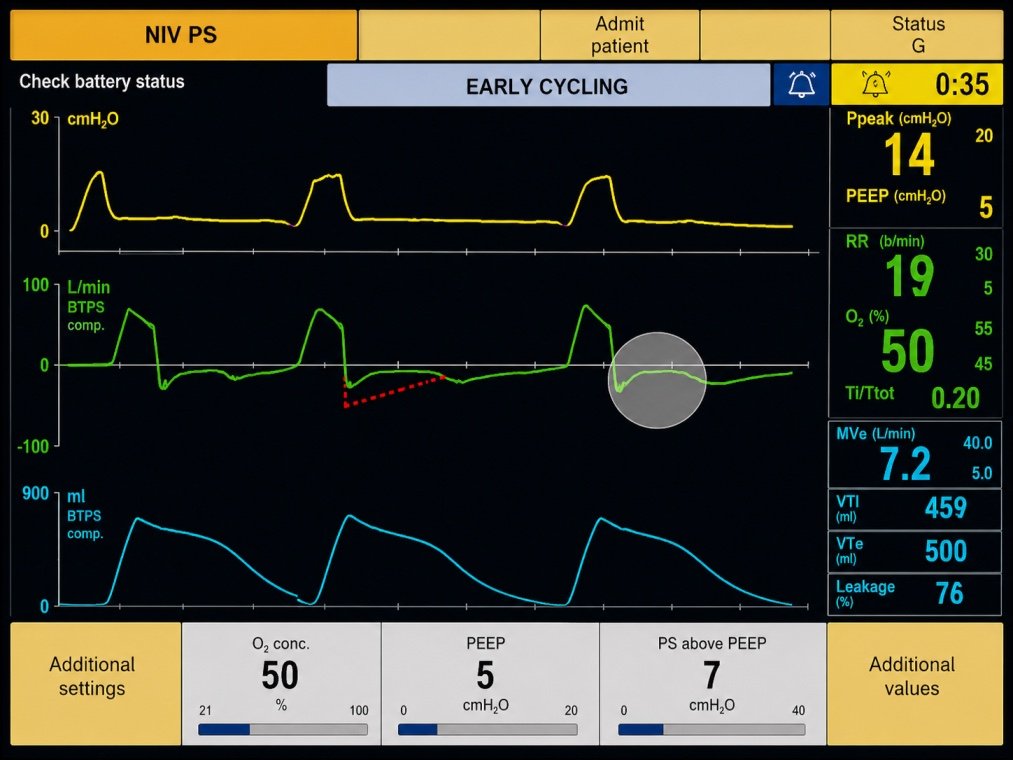
| Premature Cycling (Early Cycling-Off) |
Definition | Ventilator terminates inspiration before the patient has completed inspiratory effort. |
Mechanism | Neural inspiratory time exceeds ventilator inspiratory time. |
Causes | • High cycling threshold in PSV • Short inspiratory time • High respiratory drive • ARDS • Restrictive lung disease |
Pressure Waveform | Negative pressure deflection immediately after cycling to expiration as the patient continues to inhale. |
Flow Waveform | Persistent inspiratory effort after ventilator cycles off. |
Associated Findings | May trigger a second breath, resulting in double triggering and breath stacking. |
Management | • Lengthen inspiratory time • Lower cycling threshold (% peak inspiratory flow) • Increase pressure support if appropriate • Treat causes of high respiratory drive (pain, anxiety, acidosis, hypoxemia) |
| Delayed Cycling |
Definition | Ventilator continues inspiration after the patient wishes to exhale. |
Mechanism | Ventilator inspiratory time exceeds neural inspiratory time. |
Common In | • COPD • Pressure-support ventilation (PSV) • Excessive pressure support |
Pressure Waveform | Terminal pressure spike near end inspiration due to active expiratory effort. |
Flow Waveform | Abrupt drop in inspiratory flow as the patient attempts exhalation. |
Associated Findings | Patient may actively exhale against the ventilator. |
Management | • Shorten inspiratory time • Increase cycling threshold (earlier cycling) • Reduce pressure support • Optimize settings in obstructive lung disease • Improve patient–ventilator synchrony |