
Cervical Spine injury
Table of Contents
ToggleEtiology
1. Traumatic Causes (≈80%)
- Motor vehicle accidents (most common)
- Falls (especially in elderly)
- Sports injuries
- Violence (gunshot, stab wounds)
- Industrial accidents
2. Non-traumatic Causes
- Tumors (intramedullary/extramedullary)
- Infections (TB, epidural abscess)
- Ischemia/infarction (e.g., aortic surgery)
- Degenerative diseases (cervical spondylotic myelopathy)
- Inflammatory (transverse myelitis, MS)
Anatomy
|
Region |
Vertebral Levels |
Function Loss |
|
Cervical (C1–C8) |
Neck |
Quadriplegia, respiratory failure (C3–C5 affects diaphragm) |
|
Thoracic (T1–T12) |
Chest |
Paraplegia, loss of intercostal function |
|
Lumbar (L1–L5) |
Lower back |
Paraplegia, bladder/bowel involvement |
|
Sacral (S1–S5) |
Pelvis |
Bowel, bladder, sexual dysfunction |
Neurological Level of Injury
The neurological level of injury (NLI) is defined as the most caudal spinal cord segment in which motor and sensory functions remain intact. Clinically, this corresponds to the lowest level demonstrating at least antigravity muscle power (Medical Research Council grade ≥3/5) together with preserved sensation to both light touch and pinprick.
It is important to recognize that the neurological level does not always correspond precisely to the anatomical site of spinal column injury identified on imaging, as spinal cord dysfunction may extend above or below the radiographic level of injury.
Example 1: Cervical Spine Injury
A patient is involved in a road traffic accident.
CT scan:Fracture-dislocation at C5 vertebra
Neurological examination:
- Deltoid (C5): 5/5
- Biceps (C5): 5/5
- Wrist extensors (C6): 3/5
- Triceps (C7): 0/5
- Normal sensation up to C6 dermatome
- Sensation absent below C6
Neurological level = C6
Although the fracture is at the C5 vertebral level, the neurological level is C6 because C6 is the lowest segment with preserved motor and sensory function.
Example 2: Thoracic Injury
MRI:Burst fracture of T10 vertebra
Clinical examination:
- Normal sensation to T8 dermatome
- Sensation impaired from T9 downward
- Lower limb weakness
Neurological level = T8
Here, the anatomical injury is at T10 vertebra, but the neurological level is T8 because the spinal cord dysfunction extends above the vertebral injury.
Mechanism of Injury
Primary Injury
- Occurs at the moment of trauma
- Direct mechanical disruption of axons, neurons, and blood vessels
Secondary Injury
- Minutes to days after primary insult
- Spinal cord edema often increases over 3-6 days following the initial injury.
- Mediated by:
- Ischemia and hypoxia
- Excitotoxicity (glutamate release)
- Free radical formation
- Inflammatory cytokines
- Edema → ↑ Intramedullary pressure → further ischemia
Classification Systems
1. Anatomical Classification
- Complete SCI – No motor/sensory function below lesion, including S4–S5
- Incomplete SCI – Some sensory/motor sparing below lesion
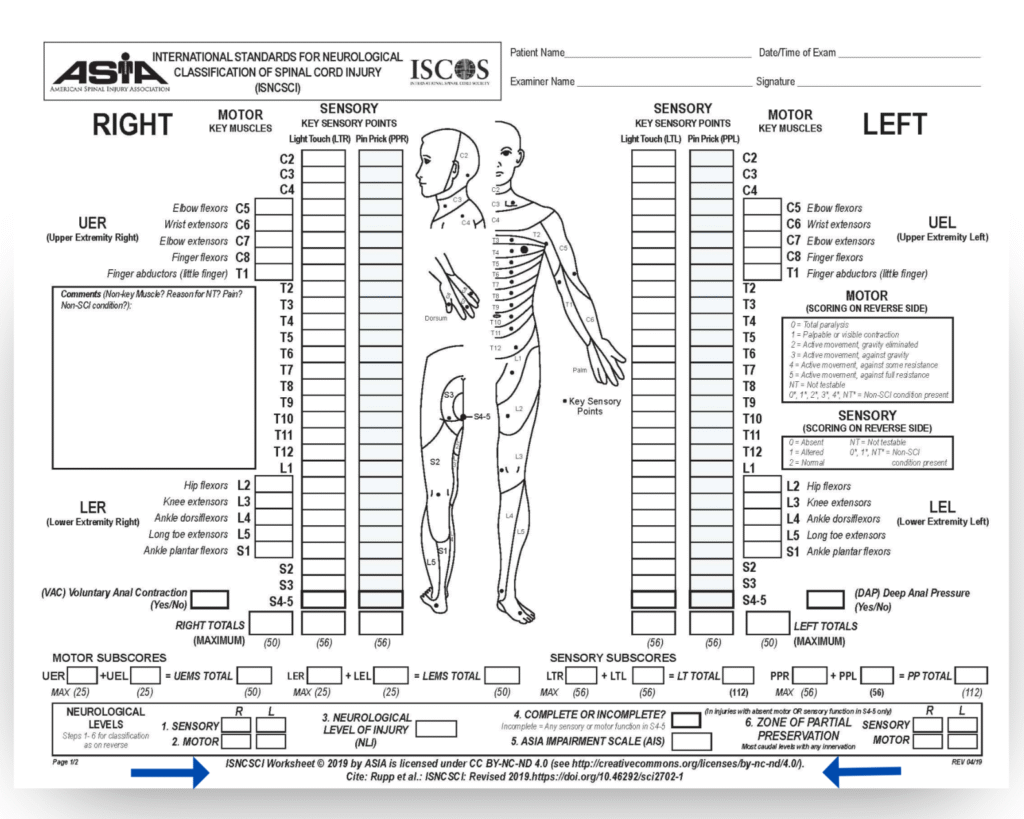
2. ASIA Impairment Scale (American Spinal Injury Association)
|
Grade |
Description |
|
A |
Complete – no motor/sensory below level, including sacral |
|
B |
Sensory incomplete – sensory preserved, no motor below |
|
C |
Motor incomplete – motor preserved, but <50% of key muscles have grade ≥3 |
|
D |
Motor incomplete – ≥50% of key muscles have grade ≥3 |
|
E |
Normal – motor and sensory normal |
Syndromic Classification (Incomplete Injuries)
|
Syndrome |
Mechanism |
Clinical Features |
|
Central Cord Syndrome |
Hyperextension injury (elderly, cervical spondylosis) |
Greater weakness in upper limbs > lower limbs, bladder dysfunction, variable sensory loss |
|
Anterior Cord Syndrome |
Flexion or anterior spinal artery infarct |
Loss of motor, pain, and temperature below lesion; preserved proprioception |
|
Posterior Cord Syndrome |
Rare (posterior spinal artery infarct, B12 deficiency) |
Loss of proprioception and vibration, preserved motor and pain/temp |
|
Brown-Sequard Syndrome |
Hemisection (stab, gunshot) |
Ipsilateral motor + proprioception loss, contralateral pain/temp loss |
|
Conus Medullaris Syndrome |
Injury at L1 level |
Early bladder, bowel, sexual dysfunction, symmetrical motor weakness |
|
Cauda Equina Syndrome |
Injury to lumbosacral roots |
Asymmetric weakness, areflexia, saddle anesthesia, severe radicular pain |
Clinical Features
1. Motor and Sensory Loss
- Below level of lesion
- Determined by dermatomal and myotomal mapping
2. Autonomic Dysfunction
- Neurogenic shock (acute phase)
- Hypotension, bradycardia, warm dry skin
- Loss of sympathetic tone (T1–L2)
- spinal cord damage above the T6 level will cause a selective deficit of sympathetic innervation of the heart (causing the heart to receive unopposed parasympathetic activity from the vagus nerve).
- Autonomic dysreflexia (chronic phase)
- Lesions above T6
- Triggered by bladder distension, bowel impaction, pain
- Severe hypertension with reflex bradycardia
3. Respiratory Compromise
- C3–C5: Diaphragmatic paralysis (phrenic nerve)
- C5–T6: Weak intercostal muscles
4. Bladder and Bowel Dysfunction
- Above sacral segments: Spastic (reflex) bladder
- Below sacral segments: Atonic (flaccid) bladder
Neurogenic vs Spinal Shock
|
Feature |
Spinal Shock |
Neurogenic Shock |
|
Cause |
Loss of spinal reflexes below lesion(reversible impairment) |
Loss of sympathetic tone |
|
Onset |
Immediately after injury |
Usually in cervical/high thoracic(above T6)-selective removal of sympathetic |
|
Duration |
Days to weeks(it has 4 phases) |
Hours to days |
|
BP |
Variable(Normal or low) |
Hypotension(due to vasodilation) |
|
HR |
Normal or variable |
Bradycardia>>normal HR |
|
Other |
Phase 1 (0–24 hours) Areflexia/Hyporeflexia Features:Complete loss of reflexes,Flaccid paralysis,Loss of autonomic activity. Phase 2 (1–3 days) Initial Reflex Return Earliest reflexes return:Delayed plantar response,Bulbocavernosus reflex (BCR) Phase 3 (1–4 weeks) Early Hyperreflexia Features:Reflexes become brisk,Muscle tone increases Phase 4 (1–12 months) Spasticity andHyperreflexia Features:Hypertonia,Clonus,Spastic paralysis. |
|
|
Reflexes |
Absent |
Intact above lesion |
|
End point |
Return of bulbocavernosus reflex |
Hemodynamic stabilization |
|
Management |
no specific treatment for spinal shock itself.Management focuses on acute SCI. |
vasopressors +/- inotropes i.e (e.g., epinephrine monotherapy, or a combination of norepinephrine plus dobutamine |
Diagnostic Evaluation
|
Investigation |
Purpose |
|
X-ray (spine) |
Initial screening for fracture/dislocation |
|
CT scan |
Bony detail, canal compromise |
|
MRI (spine) |
Gold standard for cord edema, hemorrhage, compression |
|
Neurological exam (ASIA) |
Baseline grading |
|
Urodynamic study |
For chronic bladder dysfunction |
Clinical Clearance of Cervical Spine: NEXUS vs Canadian C-Spine Rule
Both are validated decision-making tools to safely avoid unnecessary imaging in trauma patients who are alert, cooperative, and hemodynamically stable.
1. NEXUS Criteria (National Emergency X-Radiography Utilization Study)
Purpose:
To identify low-risk patients in whom cervical spine injury can be excluded clinically — no imaging required if all criteria are negative.
NEXUS Low-Risk Criteria
Imaging is NOT needed if the patient has all five of the following:
|
Criterion |
Explanation |
|
1. No midline cervical tenderness |
No pain on palpation over cervical spine spinous processes |
|
2. No focal neurological deficit |
No motor or sensory deficit |
|
3. Normal level of alertness |
GCS = 15, oriented ×3 |
|
4. No intoxication |
No alcohol or drug influence affecting evaluation |
|
5. No painful distracting injury |
No major injury (e.g., long bone fracture, visceral injury) diverting attention from neck pain |
If all 5 criteria are met → No imaging required.
If any one is positive → CT cervical spine (preferred).
Performance
- Sensitivity: ~99.6%
- Specificity: ~12%
- Advantages: Simple, quick, easy to apply
- Limitations: Low specificity → over-imaging possible
2. Canadian C-Spine Rule (CCR)
Purpose:To identify trauma patients who require imaging after blunt trauma to the head/neck.
Applies to:
- Alert (GCS 15)
- Stable vital signs
- Blunt trauma mechanism
Step 1: Any High-Risk Factor → Imaging Needed
|
High-Risk Factor |
Example |
|
Age ≥ 65 years |
Elderly fall, minor trauma |
|
Dangerous mechanism |
Fall > 1 m / 5 stairs, axial load (diving), high-speed MVC (>100 km/h), rollover, ejection |
|
Paresthesias in extremities |
Sensory symptoms indicating cord involvement |
If yes → imaging required
If no → proceed to Step 2
Step 2: Any Low-Risk Factor → Safe Assessment of ROM
|
Low-Risk Factor |
Meaning |
|
Simple rear-end MVC |
Excluding high-speed, bus/large truck, rollover |
|
Sitting position in ED |
Not supine |
|
Ambulatory at any time |
Before or after trauma |
|
Delayed onset of neck pain |
Not immediate pain |
|
Absence of midline tenderness |
No spinal tenderness |
If none of these low-risk factors → imaging required.
If any one present → proceed to Step 3.
Step 3: Active Neck Rotation Test
Ask the patient to actively rotate the neck 45° to both sides.
|
Finding |
Interpretation |
|
Able to rotate 45° both sides |
No imaging needed |
|
Unable to rotate |
Imaging required |
Performance
- Sensitivity: 99–100%
- Specificity: 42–45% (higher than NEXUS)
- Advantages: More specific, reduces unnecessary imaging
- Limitations: Slightly complex, not for <16 years or GCS <15
Emergency Management (ATLS-Based)
1. Airway, Breathing, Circulation (ABC)
- Assume C-spine injury in all trauma until ruled out
- Airway: Jaw thrust (avoid head tilt–chin lift)
- Intubation: Rapid sequence with Manual inline stabilization
MILS
Two commonly used techniques include:
- The assistant may kneel beside the operator and stabilize the head by holding the mastoid regions or supporting the occiput with both hands.
- Alternatively, the assistant may stand at the head end facing the operator, placing both hands along the sides of the patient’s head while resting the forearms on the patient’s chest to maintain alignment.
- Once the airway has been successfully secured, MILS should be discontinued and replaced with definitive cervical spine immobilization using a rigid cervical collar along with lateral supports (foam blocks or sandbags) and securing straps across the forehead and chin.
- For emergency tracheal intubation, the use of a bougie-assisted technique is recommended as the preferred first-line approach, whether direct laryngoscopy or videolaryngoscopy is employed. An endotracheal tube mounted on a stylet may be used when a bougie is unavailable or unsuccessful.
- Awake fibre-optic intubation remains a valuable alternative in selected patients, particularly when cervical spine movement must be minimized. However, its use requires appropriate equipment, operator expertise, patient cooperation, and sufficient time; therefore, it is generally unsuitable in true airway emergencies.
Current evidence suggests that neurological worsening attributable solely to oral endotracheal intubation in patients with unstable cervical spine injuries is exceedingly uncommon. When neurological deterioration occurs after injury, it is often related to progression of the original spinal cord insult, edema, vascular compromise, or ascending myelopathy rather than airway manipulation itself.
- Breathing: Oxygen, mechanical ventilation if C3–C5 lesion
- Circulation: Avoid hypotension (MAP > 85 mmHg)
2. Immobilization
- Hard cervical collar (Philadelphia)—because of this and to avoid even lateral rotation of neck —Avoid CVC placement in internal jugular vein.
- If possible try to Avoid removing soft Collar while Intubating.hard collars should not be used during airway management.hard collars also limit mouth opening
- Spine board with logroll precautions
3. Pharmacologic Management
- High-dose methylprednisolone – Controversial
- NASCIS II suggested benefit if started within 8 hours
- Current guidelines (AANS, 2021): Not routinely recommended due to infection, GI bleed, hyperglycemia.
4. Hemodynamic Goals
- Maintain MAP 85–90 mmHg for first 7 days
- Avoid hypoxia and anemia (maintain Hb >10 g/dL)
- Norepinephrine first line. However, for patients with neurogenic shock and bradycardia, the use of epinephrine could be used.
5. Definitive Management
- Early surgical decompression (ideally within 24 hours)
- Indications:
- Cord compression on imaging
- Incomplete lesion with progression
- Instability or fracture dislocation
- Indications:
- Stabilisation with instrumentation/fusion
- Avoid neck movement in ICU/WARD(in post-op period) even after Stabilisation until neurosurgeon advice to remove collar.
ICU Management
|
Problem |
Management |
|
Ventilatory support |
May need prolonged ventilation therefore Early tracheostomy |
|
Vasopressor support |
Norepinephrine preferred for MAP target |
|
DVT prophylaxis |
Start within <72 hours of injury.For patients undergoing surgery, DVT prophylaxis can usually be started within 24 hours of surgery, but this decision should be made jointly with the surgical team. |
|
Pressure sore prevention |
Regular repositioning, air mattress |
|
Bladder management |
Intermittent or indwelling catheterization |
|
Bowel management |
Stool softeners, digital stimulation |
|
Nutritional support |
High-protein diet for wound healing |
|
Physiotherapy & rehabilitation |
To prevent contractures, maintain mobility |
|
Psychological support |
Depression and anxiety are common |
|
Temperature regulation |
Poikilothermia due to loss of sympathetic control
|
|
Autonomic dysreflexia |
Treat with sitting up, remove triggers, give nifedipine/labetalol
|
|
Infection risk |
Especially pneumonia and UTI
|
|
Spasticity control |
Baclofen, tizanidine
|
|
Pain management |
Neuropathic (gabapentin, pregabalin)
|
Prognostic Indicators
|
Good Prognosis |
Poor Prognosis |
|
Incomplete lesion |
Complete lesion |
|
Early return of reflexes |
No improvement in 72 hours |
|
Early decompression |
Associated polytrauma |
|
Younger age |
Severe cord hemorrhage on MRI |
Dermatomal and Myotomal Mapping
|
Term |
Definition |
|
Dermatome |
An area of skin supplied by sensory fibers from a single spinal nerve root. |
|
Myotome |
A group of muscles innervated by motor fibers from a single spinal nerve root. |
Clinical Use:
- In spinal cord injury, assessing sensory (dermatome) and motor (myotome) levels helps determine neurological level of lesion and ASIA grading.
Dermatome Map (Sensory Distribution)
|
Spinal Level |
Area of Sensory Supply |
Bedside Clinical Landmark |
|
C1 |
No dermatome (no cutaneous branch) |
— |
|
C2 |
Back of head, upper neck |
Occipital protuberance |
|
C3 |
Side of neck |
Supraclavicular fossa |
|
C4 |
Shoulder region, clavicle |
Over acromioclavicular joint |
|
C5 |
Lateral upper arm |
Over deltoid (lateral upper arm) |
|
C6 |
Lateral forearm, thumb |
Tip of thumb |
|
C7 |
Middle finger |
Tip of middle finger |
|
C8 |
Little finger, medial forearm |
Tip of little finger |
|
T1 |
Medial upper arm |
Medial side of antecubital fossa |
|
T2 |
Axilla, upper inner arm |
Apex of axilla |
|
T3–T6 |
Upper chest |
T4 = Nipple line |
|
T7–T9 |
Lower chest, upper abdomen |
T10 = Umbilicus |
|
T11–T12 |
Lower abdomen, groin |
T12 = Inguinal ligament |
|
L1 |
Upper anterior thigh |
Just below inguinal ligament |
|
L2 |
Mid-anterior thigh |
Mid-thigh |
|
L3 |
Medial knee |
Medial femoral condyle |
|
L4 |
Medial leg and ankle |
Medial malleolus |
|
L5 |
Lateral leg, dorsum of foot |
Dorsum of foot, big toe web space |
|
S1 |
Lateral foot, sole, heel |
Lateral malleolus, little toe |
|
S2 |
Posterior thigh and calf |
Popliteal fossa |
|
S3–S5 |
Perineum |
S3–S5: saddle area, perianal region |
Myotome Map (Motor Distribution)
|
Spinal Level |
Main Muscles Tested |
Motor Function / Movement |
Key Reflex |
|
C1–C2 |
Neck flexors and extensors |
Flexion/extension of neck |
— |
|
C3 |
Trapezius, levator scapulae |
Shoulder elevation |
— |
|
C4 |
Diaphragm (phrenic nerve) |
Inspiration |
— |
|
C5 |
Deltoid, biceps |
Shoulder abduction, elbow flexion |
Biceps jerk |
|
C6 |
Biceps, wrist extensors |
Elbow flexion, wrist extension |
Brachioradialis jerk |
|
C7 |
Triceps, wrist flexors |
Elbow extension, wrist flexion |
Triceps jerk |
|
C8 |
Finger flexors, small hand muscles |
Finger flexion/grip |
— |
|
T1 |
Interossei, intrinsic hand muscles |
Finger abduction/adduction |
— |
|
T2–T12 |
Intercostals, abdominal muscles |
Trunk stability, respiration |
— |
|
L1–L2 |
Iliopsoas |
Hip flexion |
— |
|
L3 |
Quadriceps |
Knee extension |
Patellar (knee) jerk |
|
L4 |
Tibialis anterior |
Ankle dorsiflexion |
Knee jerk (also L3) |
|
L5 |
Extensor hallucis longus, gluteus medius |
Great toe extension, hip abduction |
— |
|
S1 |
Gastrocnemius, soleus |
Plantar flexion |
Ankle jerk |
|
S2 |
Hamstrings |
Knee flexion |
— |
|
S3–S5 |
Anal sphincter, pelvic floor |
Anal tone, bladder/bowel control |
Anal wink / bulbocavernosus reflex |
Clinical Correlation Table
|
Spinal Level |
Motor Deficit |
Sensory Loss |
Reflex Change |
|
C5 |
Weak shoulder abduction, elbow flexion |
Lateral arm |
↓ Biceps reflex |
|
C6 |
Weak wrist extension |
Thumb, lateral forearm |
↓ Brachioradialis |
|
C7 |
Weak elbow extension |
Middle finger |
↓ Triceps reflex |
|
C8 |
Weak grip |
Little finger, medial forearm |
— |
|
L3–L4 |
Weak knee extension |
Medial leg |
↓ Knee jerk |
|
L5 |
Weak great toe extension |
Dorsum of foot |
— |
|
S1 |
Weak plantar flexion |
Lateral foot |
↓ Ankle jerk |
Clinical Application in Spinal Cord Injury (SCI)
- Determine sensory level (lowest dermatome with intact sensation)
- Determine motor level (lowest myotome with MRC ≥3/5)
- The neurological level of injury = lower of sensory and motor levels.
- Complete lesion: No S4–S5 sensory or motor function (no anal sensation or tone)
- Incomplete lesion: Any sacral sparing (e.g., preserved perianal sensation or voluntary anal contraction)
- Always test sensation symmetrically (light touch + pinprick).
- Use MRC grading for motor power (0–5 scale).
- Examine deep tendon reflexes and anal tone.
- Document level as:
e.g. C6 AIS B → C6 level, sensory incomplete.
References
- Irwin and Rippe’s Intensive Care Medicine. Spinal cord injury and neurocritical care chapters.
- Oh’s Intensive Care Manual. Neurologic emergencies and spinal cord injury.
- ISCCM Textbook Of Critical Care 2026